
To evaluate the ability of a commercialized deep learning reconstruction technique to depict intracranial vessels on the brain computed tomography angiography and compare the image quality with filtered-back-projection and hybrid iterative reconstruction in terms of objective and subjective measures. Forty-three patients underwent brain computed tomography angiography, and images were reconstructed using three algorithms: filtered-back-projection, hybrid iterative reconstruction, and deep learning reconstruction. The image noise, computed tomography attenuation value, signal-to-noise ratio, and contrast-to-noise ratio were measured in the bilateral cavernous segment of the internal carotid artery, vertebral artery, basilar apex, horizontal segment of the middle cerebral artery and used for the objective assessment of the image quality among the three different reconstructions. The subjective image quality score was significantly higher for the deep learning reconstruction than hybrid iterative reconstruction and filtered-back-projection images. The deep learning reconstruction markedly improved the reduction of blooming artifacts in surgical clips and coiled aneurysms. The deep learning reconstruction method generally improves the image quality of brain computed tomography angiography in terms of objective measurement and subjective grading compared with filtered-back-projection and hybrid iterative reconstruction. Especially, deep learning reconstruction is deemed advantageous for better depiction of small vessels compared to filtered-back projection and hybrid iterative reconstruction.
Brain multidetector-row Computed Tomography Angiography (CTA) is a suitable noninvasive imaging modality frequently used in cases of vascular diseases including aneurysm, vessel dissection, vascular malformations, stroke, and tumors [1]. The technical improvements with high spatial and temporal resolution enabled CTA to produce comparable image quality to conventional angiography and evaluate cerebrovascular diseases, especially intracranial aneurysms [2]. However, lowering the tube voltage and currents results in a reduction of radiation exposure, which causes for degradation of image quality on CTA and affects its diagnostic accuracy. Especially the detection of small diameter vessels by CTA still presents a challenge. To visualize the intracranial vessels clearly and accurately, there should be a great deal to improve the image quality by developing image reconstruction algorithms.
Initially, hybrid iterative reconstruction (Hybrid IR) and model-based iterative reconstruction (MBIR) were effective until deep learning image reconstruction appeared on the stage. Several studies [3, 4, 5] reported that MBIR improves the delineation of small vascular structures with high image quality and spatial resolution compared to Hybrid IR. However, long reconstruction time limits its routine use in clinical practice. Clinical studies have confirmed that the low radiation dose used during hybrid iterative reconstruction and deep learning reconstruction (DLR) implies patient safety while improving image quality; additionally, lower image noise, higher contrast-to-noise ratio (CNR), and lower blooming artifacts were observed [6, 7, 8, 9].
Advancements in developing deep learning reconstruction have led to
better outcomes by low radiation exposure and excellent imaging quality. The Food
and Drug Administration has approved two artificial intelligent image
reconstruction algorithms for clinical purposes: Advanced Intelligent Clear-IQ
Engine (AiCE, Canon Medical Systems Corporation, Otawara, Japan) [10] and
TrueFidelity
 Fig. 1.
Fig. 1.Overview of deep learning reconstruction. The vast learning capacities of the deep convolutional neural network allow for differentiation between the signal and the noise. Consequently, deep learning reconstruction (DLR) reduces artifacts and noise separately from the signal. AiCE, a DLR used in this study, was trained to use advanced model-based iterative reconstruction (MBIR) target images.
Several studies have utilized DLR in the abdominal, chest, and brain CT imaging and cardiopulmonary CTA and found better image quality than other image reconstruction algorithms [13, 14, 15, 16, 17, 18]. No studies so far have investigated the application of AiCE to brain CTA protocols. Therefore, we propose to evaluate the ability of a commercialized deep learning reconstruction technique (AiCE) to depict intracranial vessels on the brain CTA and compare the image quality with other reconstruction algorithms (FBP and Hybrid IR) in terms of objective and subjective measures.
The dose-length product (DLP) and CT dose index-volume (CTDIvol) values were collected from the dose reports.
A total of 43 consecutive patients scheduled for brain CTA from October 2020 to November 2020 were included in this study. This retrospective study was approved by the Institutional Review Board. The exclusion criteria were as follows pregnancy, allergy to iodinated contrast, and severe renal disease.
All CT examinations were performed using a 320 multi-detector row scanner
(Aquillion ONE PRISM version 10.4, Canon Medical System, Otawara, Japan) with a protocol
consisting of a tube voltage of 120 kVp, tube current of 150
mAs, field of view of 220 mm, detector collimation of 80
Images were reconstructed using three different algorithms: filtered-back projection (FBP) with FC23 kernel, hybrid iterative reconstruction (Adaptive Iterative Dose Reduction 3-D, AIDR-3D, Canon Medical Systems Corporation, Otawara, Japan) with FC23 standard kernel, and deep learning reconstruction (Advanced Intelligent Clear IQ Engine, AiCE, Canon Medical Systems Corporation, Otawara, Japan) with brain CTA standard option. The CTA images were sent to workstation (Vitrea version 7.12, Vital, Minneapolis, USA) for analysis.
Image noise, CT attenuation value (HU), Signal-to-noise ratio (SNR), and Contrast-to-noise ratio were used to objectively assess the CTA images reconstructed by FBP Hybrid IR and DLR.
Image noise was derived from the standard deviation of the HU by placing the
largest possible seven regions of interests (ROIs) in the center of the vessel
depending on the diameter of each vessel, i.e., the right and left cavernous
segments of the internal carotid artery (ICA), right and left vertebral artery,
basilar apex, and the right and left M1 segment of the middle cerebral artery
(MCA), avoiding the inclusion of the vessel wall (Fig. 2). As the reference for
contrast, another ROI (20 mm
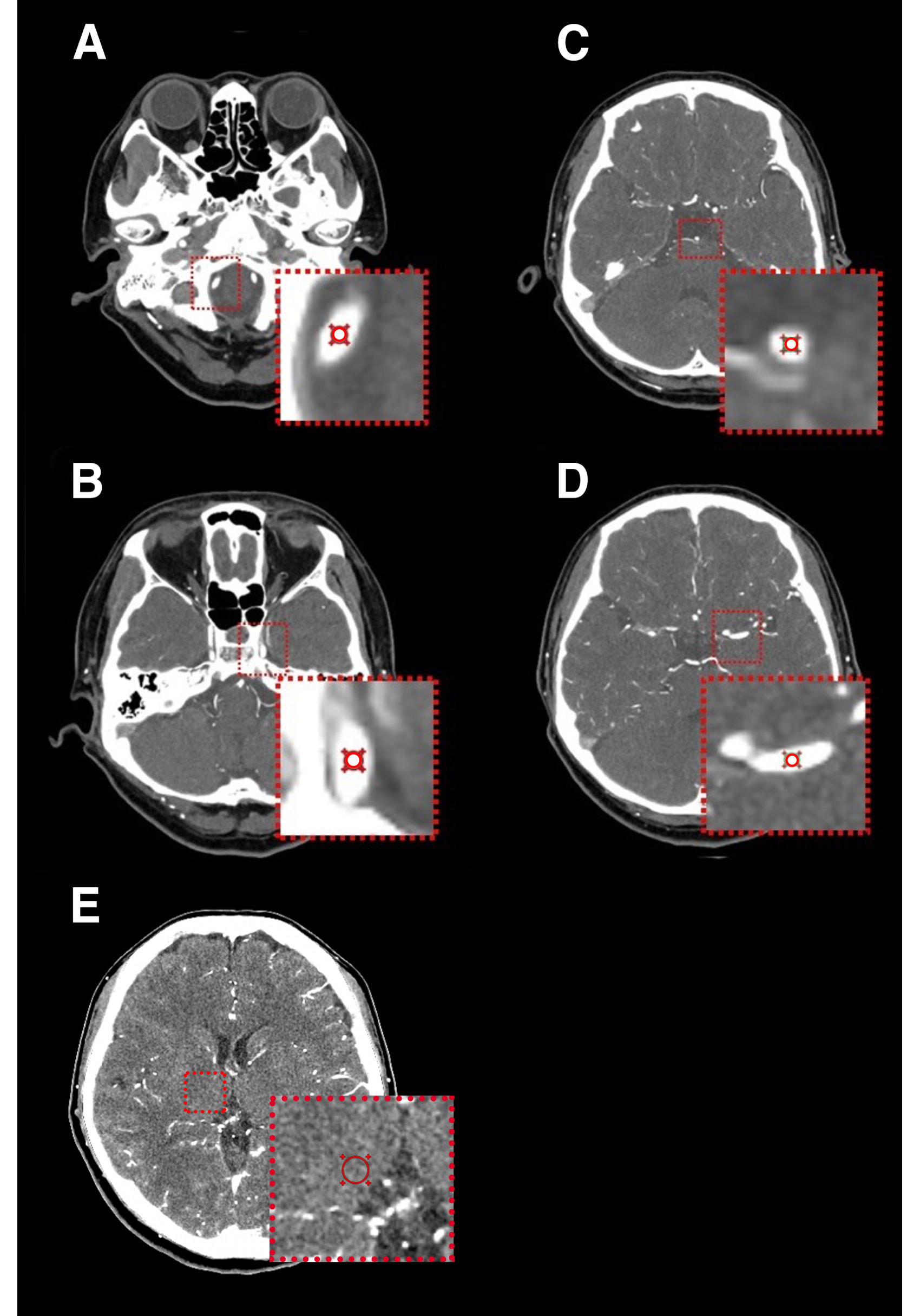 Fig. 2.
Fig. 2.Measurements of objective image quality in the brain CTA. The region of interest (ROI) was placed in the center of the right and left vertebral artery (A), basilar apex (B), right and left cavernous segment of the internal carotid artery (C), right and left M1 segments of the middle cerebral artery (D), and right thalamic gray matter (E) avoiding the inclusion of a vessel wall at the same position in the three image reconstructions with DLR, Hybrid IR, and FBP.
The SNR was assessed by dividing the attenuation of the vessels by its standard deviation. These vessels include the right and left cavernous segment of the ICA, right and left vertebral artery, basilar apex, and right and left M1 segments of the MCA.
The CNR was measured as the contrast divided by the noise strength. The contrast was difference between CT attenuation of the vessels and the attenuation of the thalamic gray matter. The vessels include the right and left cavernous segments of the ICA, right and left vertebral arteries, basilar apex, and right and left M1 segments of the MCA.
The surgical clips’ sharpness and aneurysm coils were assigned with their perimeter and 10–90% edge rise distance (ERD) on FBP, Hybrid IR, and DLR. The perimeter of surgical clips and aneurysm coils was analyzed by manual placement of an electronic caliper on the workstation (Vitrea, Vital, Minneapolis, USA). On axial images, the CT attenuation profile with a horizontal line through the center of the clip and coil was determined in the same location for all reconstruction methods. The 10–90% ERD was considered the distance of 10% and the 90% of the peak CT attenuation number. The mean value of three measurements was used for analysis. A shorter edge rise distance demonstrates a higher sharpness. To assess the sharpness of the surgical clips and aneurysm coils, normalized profile curves were compared in the images reconstructed with FBP, Hybrid IR, and DLR using ImageJ software (version 3.0, LOCI, University of Wisconsin, Madison, Wisconsin, USA) [19].
The images were subjectively evaluated by two neuroradiologists (each with reading experience longer than five years). The neuroradiologists were blinded to the image reconstruction methods and randomly evaluated the CTA images. A five-point Likert scale was used for the analysis: 5 = excellent image quality, exquisite vessel delineation wall with barely perceived image noise; 4 = good image quality, good vessel delineation wall with minimal image noise; 3 = acceptable image quality, moderate vessel delineation wall with moderate image noise; 2 = suboptimal image quality, fair vessel sharpness and vessel delineation wall with severe image noise; and 1 = poor limited image quality, limitation in the vessel wall delineation with excessive image noise.
Continuous variables were shown as mean
The mean DLP was 219.05
Forty-three patients were included in the study (19 were male (55.8%), and 24
were female (44.2%)). Their mean age was 56.77
The objective analysis findings of the FBP, Hybrid IR, and DLR are shown in
Tables 1,2. In all patients, the average noise was 19.80
| The mean value |
p-value | ||||||
| FBP | Hybrid IR | DLR | FBP vs Hybrid IR vs DLR | FBP vs Hybrid IR | FBP vs DLR | Hybrid IR vs DLR | |
| Image noise (HU) | |||||||
| Thalamus | 14.71 |
9.92 |
9.00 |
0.001 | 0.001 | 0.001 | 0.001 |
| ICA right | 19.16 |
15.89 |
11.16 |
0.001 | 0.001 | 0.001 | 0.001 |
| ICA left | 19.71 |
16.87 |
11.87 |
0.001 | 0.001 | 0.001 | 0.001 |
| VA right | 19.87 |
16.32 |
9.65 |
0.001 | 0.001 | 0.001 | 0.001 |
| VA left | 19.26 |
16.03 |
10.09 |
0.001 | 0.001 | 0.001 | 0.001 |
| BA apex | 20.73 |
17.85 |
11.23 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA right | 23.37 |
20.14 |
12.59 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA left | 22.18 |
19.04 |
12.03 |
0.001 | 0.001 | 0.001 | 0.001 |
| Average | 19.80 |
16.51 |
10.95 |
0.001 | 0.001 | 0.001 | 0.001 |
| CT attenuation (HU) | |||||||
| Thalamus | 39.20 |
39.45 |
38.64 |
0.289 | 0.006 | 0.003 | 0.005 |
| ICA right | 329.03 |
327.11 |
338.27 |
0.743 | 0.001 | 0.001 | 0.001 |
| ICA left | 333.85 |
336.22 |
343.99 |
0.721 | 0.008 | 0.002 | 0.001 |
| VA right | 264.01 |
260.85 |
331.90 |
0.004 | 0.002 | 0.001 | 0.001 |
| VA left | 271.86 |
269.37 |
314.66 |
0.010 | 0.001 | 0.001 | 0.001 |
| BA apex | 258.07 |
242.03 |
310.02 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA right | 304.44 |
302.19 |
347.65 |
0.017 | 0.001 | 0.001 | 0.001 |
| MCA left | 293.40 |
289.11 |
341.08 |
0.007 | 0.001 | 0.001 | 0.001 |
| Average | 261.73 |
259.54 |
295.78 |
0.001 | 0.001 | 0.001 | 0.001 |
| FBP, filtered back projection; Hybrid IR, hybrid iterative reconstruction; DLR, deep learning reconstruction; ICA, internal carotid artery; VA, vertebral artery; BA, basilar artery; MCA, middle cerebral artery. | |||||||
| The mean value |
p-value | ||||||
| FBP | Hybrid IR | DLR | FBP vs Hybrid IR vs DLR | FBP vs Hybrid IR | FBP vs DLR | Hybrid IR vs DLR | |
| SNR | |||||||
| ICA right | 18.14 |
22.76 |
33.03 |
0.001 | 0.001 | 0.001 | 0.001 |
| ICA left | 18.25 |
22.14 |
32.36 |
0.001 | 0.001 | 0.001 | 0.001 |
| VA right | 14.74 |
17.52 |
38.98 |
0.001 | 0.001 | 0.001 | 0.001 |
| VA left | 15.31 |
18.53 |
36.09 |
0.001 | 0.001 | 0.001 | 0.001 |
| BA apex | 13.98 |
16.51 |
32.85 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA right | 14.95 |
18.05 |
34.15 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA left | 13.99 |
16.76 |
32.53 |
0.001 | 0.001 | 0.001 | 0.001 |
| Average | 13.51 |
16.28 |
30.27 |
0.001 | 0.001 | 0.001 | 0.001 |
| CNR | |||||||
| ICA right | 15.99 |
20.02 |
29.27 |
0.001 | 0.001 | 0.001 | 0.001 |
| ICA left | 16.13 |
19.54 |
28.73 |
0.001 | 0.001 | 0.001 | 0.001 |
| VA right | 12.54 |
14.84 |
34.45 |
0.001 | 0.001 | 0.001 | 0.001 |
| VA left | 13.09 |
15.80 |
31.72 |
0.001 | 0.001 | 0.001 | 0.001 |
| BA apex | 11.85 |
13.92 |
28.80 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA right | 12.92 |
15.49 |
30.13 |
0.001 | 0.001 | 0.001 | 0.001 |
| MCA left | 12.03 |
14.35 |
28.83 |
0.001 | 0.001 | 0.001 | 0.001 |
| Average | 15.62 |
18.90 |
34.28 |
0.001 | 0.001 | 0.001 | 0.001 |
| FBP, filtered back projection; Hybrid IR, hybrid iterative reconstruction; DLR, deep learning reconstruction; ICA, internal carotid artery; VA, vertebral artery; BA, basilar artery; MCA, middle cerebral artery; CNR, contrast-to-noise ratio; SNR, signal-to-noise ratio. | |||||||
There was no significant difference in the attenuation of the thalamus and right
and left cavernous segments of the ICA among all image reconstruction methods. On
the other hand, the attenuation of the bilateral vertebral arteries, basilar
apex, and the bilateral M1 segments of the MCA were significantly higher in DLR
than in FBP and Hybrid IR (all p
The CNR was significantly higher in the DLR than in Hybrid IR and FBP for all
patients (p
Similarly, the SNR was significantly higher in the DLR than in Hybrid IR and
FBP, representing an average increase in the SNR by 46.22% (DLR vs Hybrid IR)
and 55.37% (DLR vs FBP, p
The perimeter for coiled aneurysm and the surgical clip resulted in 3.93
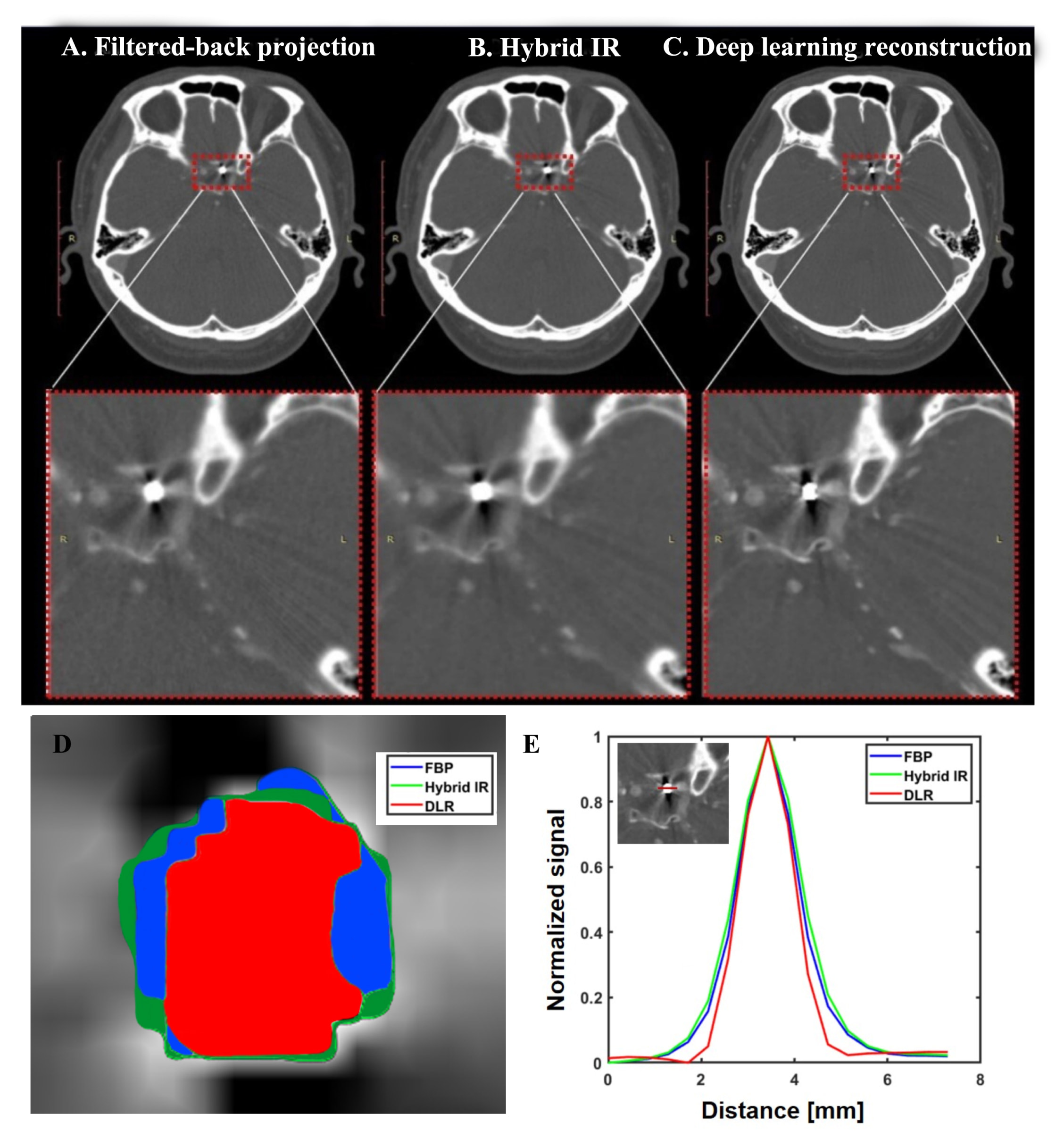 Fig. 3.
Fig. 3.Examples of brain CTA scan for a coiled aneurysm in the left paraclinoid internal carotid artery. The blooming artifact from coiling reduced in the deep learning reconstruction (DLR) (C) compared to filtered-back projection (FBP) (A) and hybrid iterative reconstruction (IR) (B). The coiling part can be seen on the magnified images with the red dashed outline for FBP, Hybrid IR, and DLR. Deep learning reconstruction was rated 3 scores, while the hybrid iterative and filtered-back projection were rated 2 by objective 2. The reduction blooming artifact and image sharpness were markedly improved in the deep learning reconstruction than FBP and Hybrid IR in terms of the perimeter (D) and normalized profile curve of 10–90% edge rise distance (E).
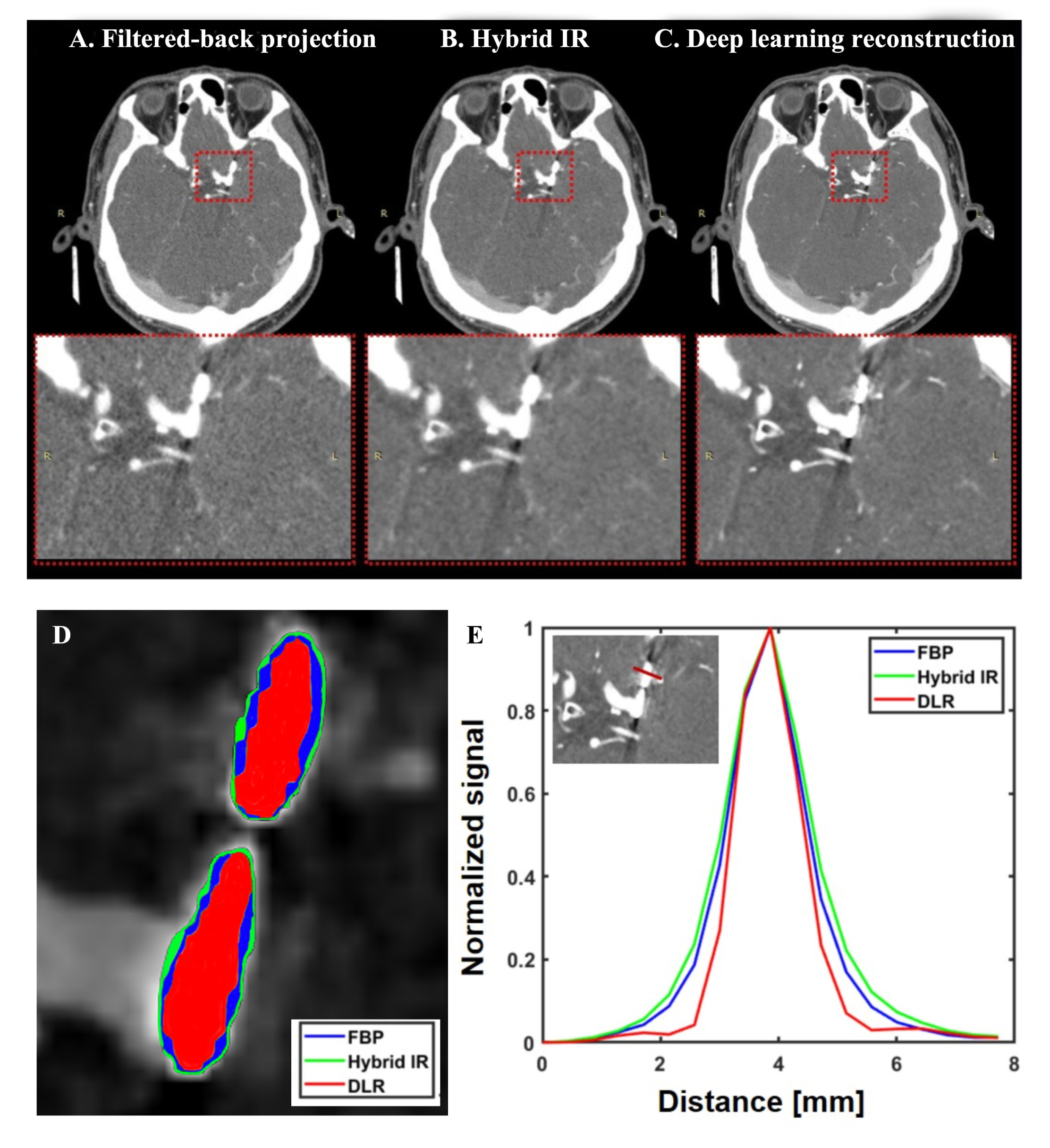 Fig. 4.
Fig. 4.Examples of brain CT angiographic scan for surgically clipped left paraclinoid aneurysms. The blooming artifact from surgically clips decreased in the deep learning reconstruction (DLR) (C) than hybrid iterative reconstruction (IR) (B) and filtered-back projection (FBP) (A). The surgical clip can be seen on the magnified images with the red dashed outline for FBP, Hybrid IR, and DLR. The subjective score of images qualified from two observers on deep learning reconstruction (score 4) was higher than hybrid iterative reconstruction (score 3) and filtered back projection (score 3). The use of DLR resulted in sharper images with reduction of blooming artifact compared to FBP and Hybrid IR when considering the analysis of perimeter (D) and normalized profile curve of 10–90% edge rise distance (E).
The subjective image quality scores of DLR were significantly higher than those
of the Hybrid IR and FBP (p
| FBP | Hybrid IR | DLR | p-value | ||||
| FBP vs Hybrid IR vs DLR | FBP vs Hybrid IR | FBP vs DLR | Hybrid IR vs DLR | ||||
| Observer 1 | |||||||
| Overall image quality | 2.14 |
3.26 |
3.46 |
0.001 | 0.001 | 0.001 | 0.02 |
| Observer 2 | |||||||
| Overall image quality | 2.23 |
3.30 |
3.49 |
0.001 | 0.001 | 0.001 | 0.074 |
| FBP, filtered back projection; Hybrid IR, hybrid iterative reconstruction; DLR, deep learning reconstruction. | |||||||
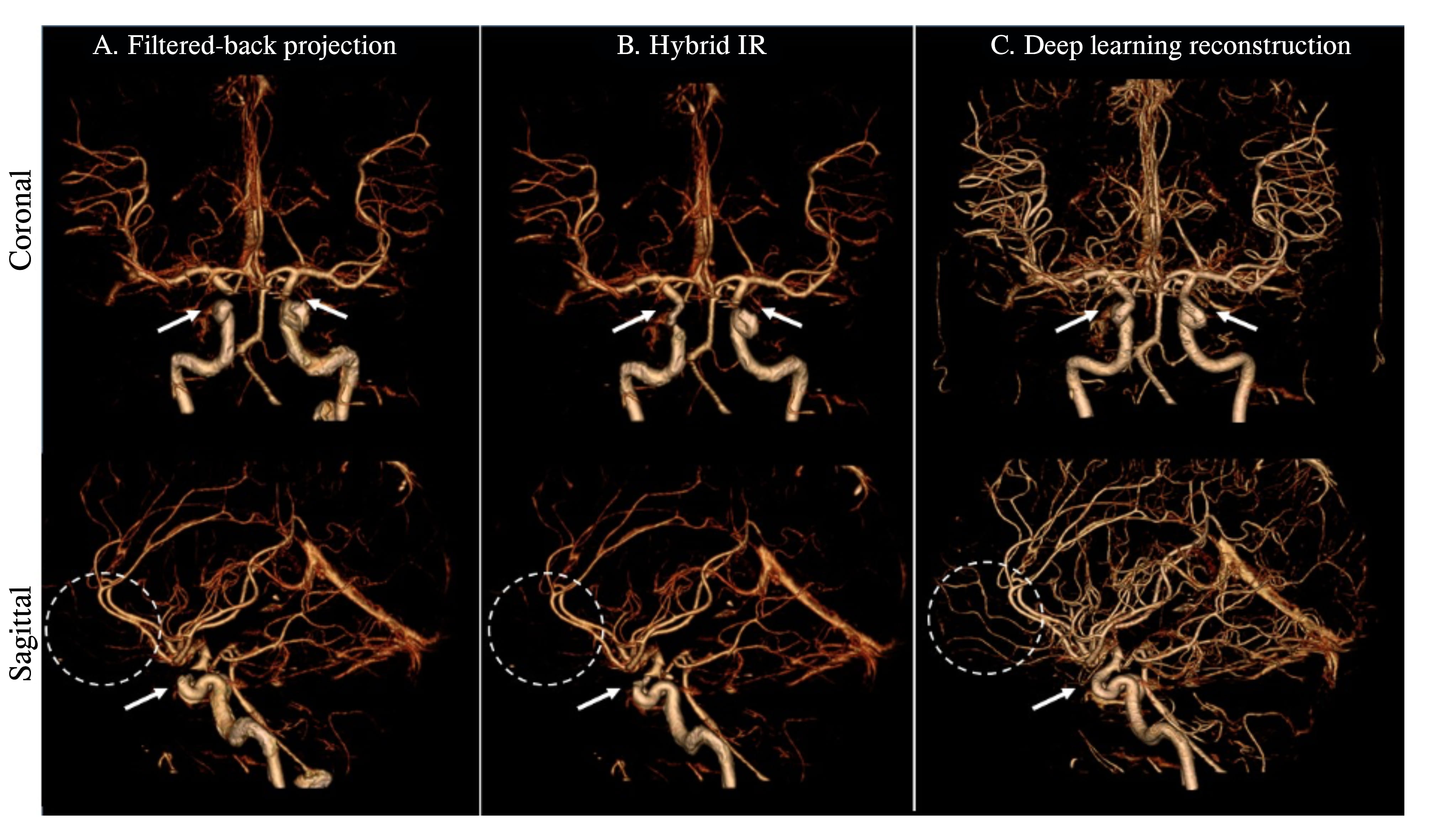 Fig. 5.
Fig. 5.Volume rendering of brain vessels extracted by bone removal from only CTA images. The volume-rendered image of brain CTA using deep learning reconstruction (C) shows an increased number of cortical branches and completeness of clinoid and supraclinoid segments of ICA (white arrows) compared to hybrid iterative (B) and filtered back projection (A). In addition, deep learning reconstruction allows more conspicuous visualization of the major terminal branches, including frontobasal and frontopolar arteries (dashed circle). At the same time, they are not seen in the hybrid iterative reconstruction (IR) and filtered back projection. Deep learning reconstruction provided significantly greater enhancement on small cortical branches of brain arteries, resulting in markedly improved vascular visualization. The images were views in the same window level and width.
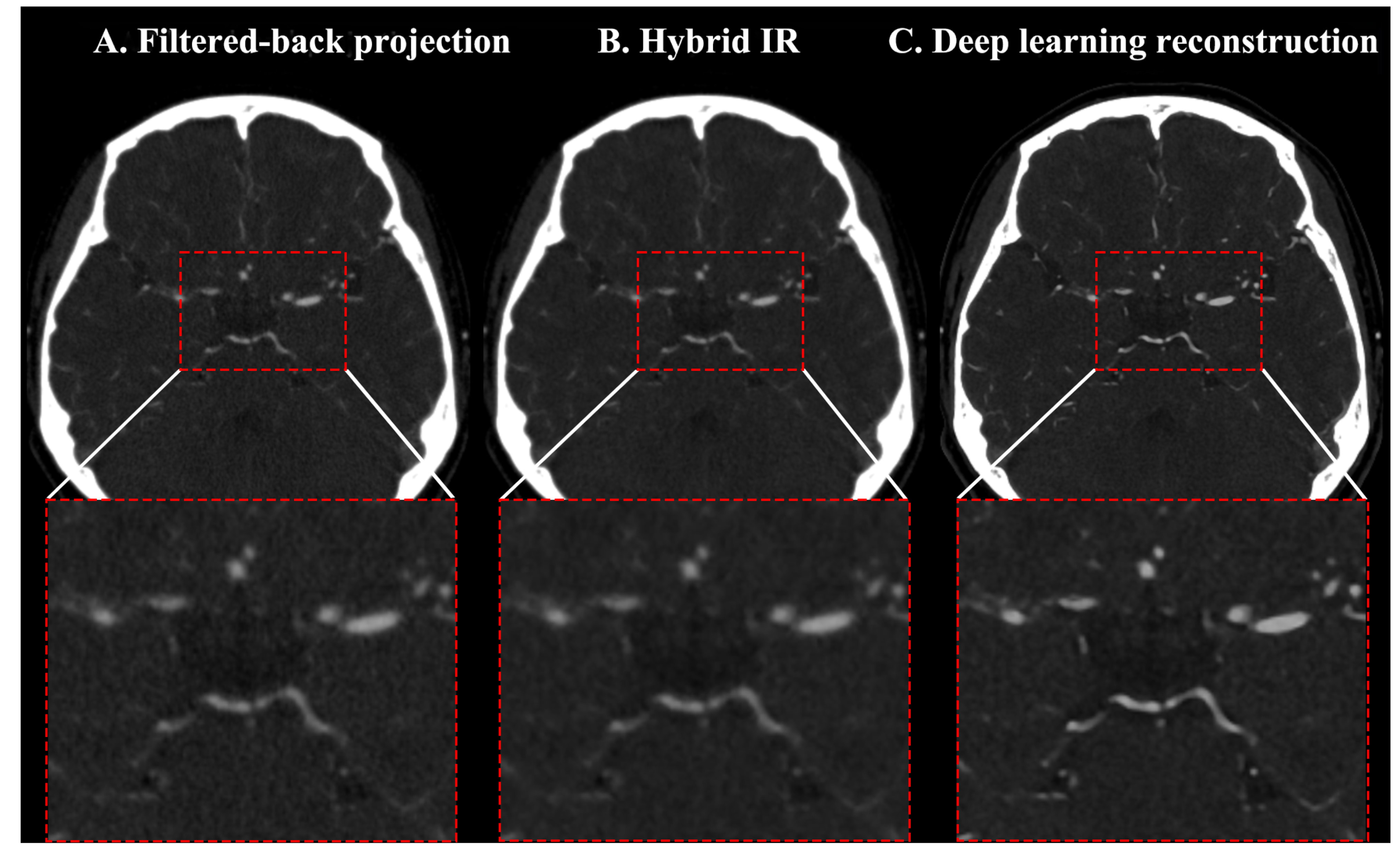 Fig. 6.
Fig. 6.Axial cut brain CTA images for visualization of intracranial vessel. Comparison of brain CTA between filtered-back projection (A), hybrid iterative reconstruction (IR) (B), and deep learning reconstruction (C) in the vessel visualization. The deep learning reconstructions (C) demonstrated a good vessel delineation wall with minimal image noise and sharp vessels compared to hybrid iterative (B) and filtered back projection (A) algorithms. The circle of Willis can be clear on the magnified images of the red dashed outlines. The image quality of the deep learning reconstruction was assessed by 4 scores, 3 scores for hybrid iterative reconstruction, and 2 scores for filtered-back projections by observer 1.
We evaluated the image quality of brain CTA using different image reconstruction algorithms, i.e., FBP, Hybrid IR, and DLR. We found that compared to Hybrid IR and FBP, DLR significantly improved objective and subjective imaging quality by reducing image noise, blooming artifacts and improving SNR and CNR. Compared to Hybrid IR and FBP, DLR has the advantage of maintaining higher image quality while minimizing the cumulative radiation exposure with low tube voltage and current [15, 21]. Recently, the fast speed reconstruction and radiation dose reduction have increased the interest in the use of DLR. Previous studies have investigated the importance of radiation dose reduction by DLR [15, 18]. The vast learning capacities of the deep convolutional neural network allow for differentiation between the signal and the noise, and consequently, DLR reduces artifacts and noise separately from the signal. AiCE, a commercialized DLR used here, was trained to the target images of advanced model-based iterative reconstruction (MBIR); additionally, it overcomes the limitations of MBIR with fast reconstruction time and improved spatial resolution and image quality [14, 22]. The reconstruction time is up to 3.5 images per sec for MBIR [15]. The reconstruction times by Hybrid IR and DLR were about 25 images per sec and 43 images per sec, which was similar to [15].
The DLR significantly reduced image noise and improved the attenuation for bilateral ICA segments, bilateral vertebral arteries, bilateral M1 segments of the MCA, and basilar apex, which led to significant improvement in the SNR and CNR. We found a 33.68% and 44.70% reduction in noise when using DLR compared to Hybrid IR and FBP. Additionally, the CNR was improved by 44.86% and 54.43% when using DLR compared to Hybrid IR and FBP, respectively. The DLR algorithm allowed an average increase in the SNR of 46.22% and 55.37% compared to Hybrid IR and FBP. No study has investigated the use of DLR in brain CTA despite previous studies investigating DLR in other body sections [13, 15, 16, 18]. Our results are consistent with previous studies investigating CT imaging of other organs [5, 13, 14, 15, 16, 17] despite the difference in location. The current and previous studies demonstrated the improved imaging quality when using DLR compared to Hybrid IR, MBIR, and FBP. We believe this improved image quality with DLR may be due to advanced MBIR images used for training DLR images. There was no significant difference in the attenuation of the right and left cavernous segments of the ICA among all image reconstruction methods. We consider that this phenomenon was caused by beam hardening artifacts in the ICA segments near the surrounding bone.
Kim et al. [16], investigating the commercialization of DLR,
TrueFidelity
Subjectively, improvements were observed in image quality when using DLR compared to FBP and Hybrid IR. According to observer 2, DLR images showed significantly better overall image quality than FBP and Hybrid IR; however, no significant difference was observed between Hybrid IR and DLR. The unfamiliar visual appearance of image features in DLR images may have affected this result, as reported previously [16, 25]. The high kVp tube voltage and variable filter kernels are the most effective approach to overcome the blooming artifacts. Unfortunately, images at high kVp tube voltage suffernlmstringname at the cost of increased radiation dose. Therefore, the image reconstruction algorithms and kernel settings are viable options to reduce the stent-related blooming artifact without exposure to high radiation doses. The reduction of blooming artifacts with DLR improved the visualization of intracranial vessels in the regions containing a surgical clip or coil. Therefore, DLR should have advantages in assessing the follow-up of aneurysms treated with flow diverters, stents, and clipping due to lower blooming artifacts. The use of DLR resulted in sharper images compared to FBP and Hybrid IR when considering analysis of 10–90% ERD and perimeter. However, hybrid iterative reconstruction reduces the blooming artifact, which is strongly related to the kernel strength [26, 27]. The result of 10–90% ERD and perimeter of the coiled aneurysm and surgical clip in FBP was similar to Hybrid IR that may be affected by reconstruction kernels used in our paper (FC23 kernel for both FBP and Hybrid IR). Therefore, the optimized reconstruction kernel is required for the reduction of blooming artifacts.
As seen in Fig. 5, the cortical segments of large vessels and the clinoid and supraclinoid segments of the ICA were well-demonstrated. The vessel completeness was the highest in the DLR, which are impacted less by noise. The use of DLR has increased the spatial resolution [28, 29]. It has been shown to significantly enhance small cortical branches of brain arteries, resulting in markedly improved vascular visualization. In addition, increasing the volume or injection rate of contrast media could enhance the small peripheral vessels. Fig. 6 illustrates that the excellent vessel delineation wall and sharp vessels were more evident in DLR than in Hybrid IR and FBP. The improvement of the spatial resolution can decrease errors in the evaluation of small vessel and carotid stenosis. Thus, the deep learning image reconstruction may be especially helpful for delineating major terminal branches, e.g., frontobasal and frontopolar arteries, and accurately estimating the grade of carotid artery stenosis. Further studies need to be done to establish these qualities of DLR as benefits in detecting vascular abnormalities, including arteriovenous fistula, abnormalities of the collateral vessels, and distal aneurysms. The DLR resulted in sharper images and reduced the blooming artifact caused by surgical clips and coiled aneurysm compared to FBP and Hybrid IR without increasing the tube voltage that leads to high radiation dose for patients. The size of the surgical clip and coiled aneurysm appeared larger than its actual size due to blooming artifacts in the FBP and Hybrid IR than DLR. The visualization of intracranial vessels in the regions containing a surgical clip or coils could be evaluated accurately with DLR.
This work has several limitations. First, this was a retrospective study that only assessed a relatively small number of patients. Second, pathologic findings were not sufficiently studied. Third, we did not compare the radiation exposure in each reconstruction method in our study. In addition, image reconstructions in this study were provided by one CT.
Furthermore, the evaluation of image quality of brain CTA with deep learning reconstruction by other vendors is needed. Lastly, the analysis of 10–90% ERD and perimeter in the surgical clip and coiled aneurysm was evaluated for only two patients and limited to coils and surgical clip types. Despite these limitations, improving vascular enhancement provides better visualization of small branches in the brain arteries without increasing the overall iodine dose delivery. As mentioned above, the image quality is improved in the deep learning reconstruction compared to filtered-back projection and hybrid iterative reconstruction.
The deep learning reconstruction method generally improves the image quality of brain CTA in terms of objective measurement and subjective grading compared with filtered back projection and hybrid iterative reconstruction methods. Especially, deep learning reconstruction is deemed advantageous for better depicting small vessels than FBP and Hybrid IR.
CTA, Computed Tomography Angiography; IR, Iterative Reconstruction; MBIR, Model-Based Iterative Reconstruction; DLR, Deep Learning Reconstruction; CNR, Contrast-to-noise ratio; FBP, Filtered-Back Projection; AiCE, Advanced Intelligent Clear-IQ Engine; SNR, Signal-to-noise ratio; ROI, Regions of interest; ICA, Internal carotid artery; MCA, Middle cerebral artery.
CO, JKR and SKK designed the research study. CO, HJS, DHH and SKK performed the research. HJS, DHH and JWS provided help and advice on the research. CO and JKR wrote the manuscript. CO and JKR analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The institutional review board of the Inje University Seoul Paik Hospital approved this retrospective study, IRB File No. 2021-06-008.
Not applicable.
This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project number: 1711139017).
The co-authors (Jae-Kyun Ryu, Seonkyu Kim) are employees of Canon Medical Systems Korea, Seoul, Korea that is the subsidiary in Korea of Canon Medical Systems Corporation, Otawara-si, Japan. The authors declare the paper has no conflicts of interest with the company.