
Social Media usage has been shown to increase in situations of natural disaster and other crises. It is crucial for the scientific community to understand how social media works in order to enhance our capabilities and make a more resilient community. Through social media communication, the scientific community can collaborate around the globe in a faster way the most important findings of a disease, with a decreased knowledge transition time to other healthcare providers (HCPs). This is greatly important to coordinate research and knowledge during a time of uncertainty and protentional fake news. During the 2020 global pandemic, social media has become an ally but also a potential threat. High volumes of information compressed into a short period can result in overwhelmed HCPs trying to discern fact from noise. A major limitation of social media currently is the ability to quickly disseminate false information which can confuse and distract. Society relies on educated scientists and physicians to be leaders in delivering fact-based information to the public. For this reason, in times of crises it is important to be leaders in the conversation of social media to guide correct and helpful information and knowledge to the masses looking for answers.
Sharing key data during a pandemic is crucial to improving patient outcomes (Almansoori and Habtoor, 2018). Social media usage has been shown to significantly increase in cases of natural disasters and crises (Gottlieb and Dyer, 2020), as information needs to be transferred quickly. This rapid dissemination overcomes barriers of traditional media into stakeholders including the public, healthcare systems and healthcare providers (HCPs) to aid in making important decisions. Formal websites, traditional journals, and e-mail have communication deficiencies that are slow in full capabilities of sharing knowledge rapidly. As a result, social media channels became the most common resource on COVID-19 for scientist and public (Gupta et al., 2020; Hermida et al., 2012). But with this bright side also comes the dark side of social media. This pandemic started an unexpected race to publish in medical journals, increasing plagiarism and poorly validated primary data (Ahmed, 2020). Most journals embarked on fast-track processing of COVID-19 submissions to prioritize and avoid delays in dissemination of potentially valuable scientific knowledge, sharing them as preprints, increasing and actively attracting social media mentions and citations by scientific community and public. At times giving a false impression of the global scholarly community approval leading to misinformation (Kwon, 2020; Callaway, 2020).
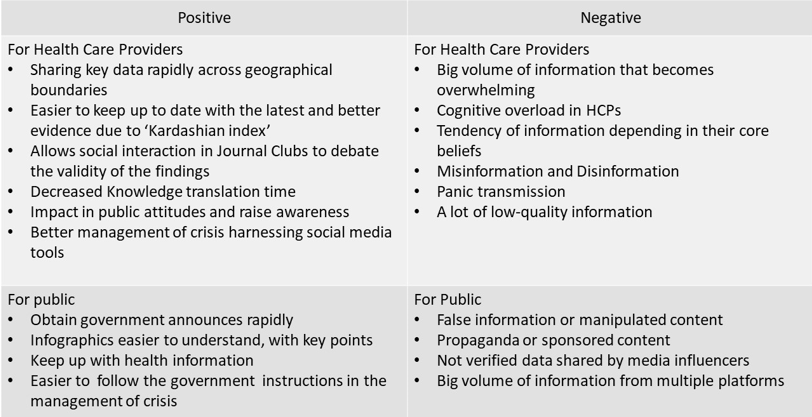
Until now, social media channels are distinguished as the most important sources of information as well as misinformation (Gupta et al., 2020) becoming our biggest ally but also our biggest enemy. See Table 1.
|
The COVID-19 pandemic is complex in nature as it has disproportionate effects on multiple groups of people. The virus is moving at varying speeds which demands the best of us and our management capabilities. Today users are harnessing social media tools to enhance organizational capacity and demonstrate resilience in response to crises. Social media users are creating new avenues for collaboration that likely will lead to more resilient communication over time (Almansoori and Habtoor, 2018).
With social media, information is shared through a network in a faster way around the globe, even faster than the pandemic virulence (Merchant and Lurie, 2020). It provides an alternative that every health care system and healthcare provider needs. To deliver quick, reliable information across geographical boundaries and time zones with clarity to address critical issues related to SARS-COV2 infection. Rapid response to the pandemic is imperative as HCPs do not have time to reflect on previous practice or rely on large scale randomized controlled trials (Kearsley and Duffy, 2020).
During a time when information changes quickly and retractions in journals occur (Mehra et al., 2020a), it is critical for health care staff to keep up to date with the latest evidence. Social media can facilitate this unmet need. As of July 22nd, 2020 there have been 34,116 articles listed in Pubmed.gov search related to SARS-COV2 infection and it is almost impossible to keep up with all this new information in addressing the crisis.
As a result, collectively many clinicians have turned away from reading journals and static internet sources and instead have turned to utilizing social media networks (Kearsley and MacNamara, 2019). Being twitter the most used platform between scientific community before pandemic (Collins et al., 2016). Social media allows for interaction in online journal clubs with experts, sharing data on a global open-source platform, bookmarking content in specified web pages, and hosting webinars and video conferences. The decreased knowledge translation time provided by social media allows HCPs to analyze and debate the literature in real-time, addressing the internal and external validity of the findings (Gottlieb and Dyer, 2020)
.Twitter has an emerging role in the dissemination of health information. There is growing evidence that a highly mentioned paper in this social platform may reflect the qualities of the paper and may be subject to a debate in journal clubs and a post publication social peer review process that might help retraction (Collins et al., 2016; Pulido et al., 2018; Eysenbach, 2011; Gross, 2016).
This plethora of social media tools has changed the landscape of crisis management considerably over recent years. Clinicians are making a faster impact in public attitudes and behaviours, (e.g. self-isolating, handwashing, accessing health care), awareness about the disease and its symptoms, and more contributions to important decisions taken during the outbreak (e.g. quarantine measures, development of new vaccines, internationally coordinated responses) (Depoux et al., 2020).
Responding to the pandemic with a well-planned analysis of global online conversations could provide a rapid assessment of the spread and prepare for surges in acuity. This may allow for advanced procurement and rationing of needed supplies to protect HCPs and patients, as well as altering hospital functions to better sustain the anticipated challenges. For example, an awareness of critical national personal protective equipment (PPE) shortages allowed for hospitals to begin to develop strategies to reallocate and ration PPE where possible and engage local businesses to repurpose production for medical supplies (Gottlieb and Dyer, 2020).
Unlike traditional broadcast news, social media is a new dynamic way to obtain information, with capacity to interact between the emisor and the receivers in an immediate way. Further examples include infographics and online debate between clinician experiences in tackling patient care. Unfortunately, the way information is found and distributed using a social media network can be challenging and overwhelming for many health workers. As an example Twitter reached a maximum volume of conversations related to COVID in one day of 548,152,410 according to the World Health Organization (WHO) (D’Agostino, 2020). The online social media tracking program TalkWalkerTM (New York City, NY, USA) reported that COVID-19 had been referenced on social media 40.2 million times from May 12th, 2020 to May 18th, 2020 (Gottlieb and Dyer, 2020).
Many experts in cardiology and nephrology have curated key websources for centralized information and content related to their fields and COVID-19. As an example the JACC journal has created a webpage dedicated to COVID and cardiology (Journal of the American College of Cardiology, 2020). NephJC.com, a respected resource for online nephrology content, has a centralized website that is continuously updated with data, publications and expert analysis relating to kidney issues in response to COVID-19 infection and the HCPs response to the pandemic (NephJC, 2020).
Social media can also be an enemy in addressing the response to a health pandemic. The volume of information is large and overwhelming and has been termed an “infodemic”. It has been reported that presenting multiple simultaneous methods of knowledge transmission introduces cognitive overload, confusion, and increases the chance of error (Leape, 1997).
There are existing platform algorithms based on the ‘Kardashian Index’, where popular threads attract higher impressions and interactions, but can lead to the spreading information that may not represent best practices (Hall, 2014; Johannsson and Selak, 2020). This could affect the flow of information because there is a tendency of individuals to connect with others who validate their core beliefs rather than be exposed to opposing viewpoints (Brennen et al., 2020).
Inside all the important late breaking data there is also misinformation and panic at the same velocity (Depoux et al., 2020). The ease through which inaccuracies and conspiracies can be repeated and perpetuated via social media and conventional outlets puts public health at a constant in the crosshairs. There may have been no way to prevent a global COVID-19 pandemic spread, but verified information is the most effective prevention against the disease of panic and misinformation (The Lancet, 2020).
Misinformation is also the result of the unexpected race to publish in medical journals, with poorly validated primary data and plagiarism (Ahmed, 2020). As an example is the evidence documenting SARS-CoV-2 myocarditis as a cause of cardiac dysfunction (Basso et al., 2020) leading to dramatic warnings in social media, suggesting a devastating impact on the myocardium. Being a statement not supported by evidence and overinterpreted (Frangogiannis, 2020). To mention another example of the seriousness of misinformation there is a report of a patient who auto medicated with several anticoagulants to give herself prophylaxis against COVID-19. She was admitted to hospital because of side effects of anticoagulation (Fernandes et al., 2020).
It is the responsibility of social media users to transfer the most trustworthy information during this period of uncertainty and squash recognized misinformation. The users are responsible for flagging fake information, so fact-checkers can help to stop the spread in the network of multiple users at the same time. This volume of flagged information related to COVID is so big that Cristina Tardáguila, Associate Director of the International Fact-checking Network (IFCN), has called COVID-19 ‘the biggest challenge fact-checkers have ever faced’.
With this context, a joint industry effort was made by media platforms against misinformation, elevating authoritative content and sharing critical updates coordinated by government healthcare agencies around the world. As examples; Twitter challenged 1.5 million accounts that were targeting COVID-19 with malicious and manipulative behavior (Gottlieb and Dyer, 2020). The WHO has created a Myth Busters Webpage to address and correct misinformation about the COVID-19 outbreak. As Facebook is being outbalanced by the number of flagged publications their fact-checkers could verify, they started using artificial intelligence with more powerful algorithms, applying its existing multimodal content analysis tools to tackle down misinformation (Sumbaly et al., 2020).
While fact-checks provide a reliable way to identify timely pieces of misinformation, fact-checkers cannot address every piece of misinformation and their professional work necessarily involves various selection biases as they focus scare resources (Brennen et al., 2020). So Analysts play another important role. The Bruno Kessler Foundation is an international company based in Italy, that helps pulling out posts with database analysis, they hold the largest database of tweets related to COVID-19. Analysts found that 40% of misinformation is posted by Bots to amplify the scope of a publication, based on the Kardashian Index. The celebrities are another important source in spreading misinformation (Fondazione Bruno Kessler, 2020). Even with this effort, there is media that can spread misinformation that is out of reach for Fact-checkers and healthcare workers like private channels, email, closed groups, and messaging apps.
Social media is essential in the way we experience news and share medical information in this pandemic. Thanks to the algorithms and tools in social media platforms, it is possible to find the most relevant information inside the colossal volume of shared knowledge, and this allows us to take actions to make an impact in public healthcare. During this time when there is a sense of urge to publish papers we have huge dilemmas over the quality, thanks to social media even in isolation the platforms allow us to interact between emisors and receivers, discussing the validity of the findings in the information shared with our network, quicker than 30 years ago.
But this positive side of social media also comes with a negative impact, the way misinformation travels is faster, hence is crucial to improve our systems understanding the flow of information between the stakeholders and do more to protect people from harmful content related to the pandemic. It is our responsibility as healthcare providers to help smashing the misinformation we found in social media, because even with artificial intelligence the fact checkers are being overwhelmed by the volume of information.
There is an opportunity to grow as scientific community, challenging our knowledge in a social medical interaction, harnessing technology that our battle with COVID-19 is providing. We must take advantages of virtual congresses (ESC Congress) associated with twitter conversations using a hashtag for information exchange. Online Journal Clubs in Twitter (@Heart_BMJ, #HeartJC), Podcasts (ESC cardio Talk, This week in cardiology) and Blogs.
By the time this editorial was being wrote there is a lack of serious data or tools to help us supporting our conclusions of how social media is changing our daily practice in this pandemic, part of the data showed was obtained from previous crises, and the pandemic is still ongoing, we are expecting more information related to chronic effects of the viral infection and we have to be aware. The adoption of careful and objective approaches for data interpretation and dissemination of scientific findings is critical to overcome the challenges of the pandemic.
All authors listed contributed equally to the research, writing, and editing of this manuscript.
The authors would like to acknowledge and thank all of the front line healthcare workers who have risked their lives and their personal health to care for so many during this COVID-19 Pandemic.
The authors declare no conflicts of interest statement.