
Academic Editor: Peter A. McCullough
Sildenafil citrate and its generic forms are widely used to treat erectile dysfunction worldwide. Sildenafil citrate associated myocardial infarction is rarely reported in patients with no previous coronary artery disease. Herein, we present a case of a 40-year-old man with no cardiovascular risk factors other than heavy smoking and heavy drinking with no known previous ischemic symptoms, who had an ST-segment elevation myocardial infarction after receiving sildenafil citrate. From this case report, we emphasize that as sildenafil is increasingly being used as a recreational drug as it is widely available without a physician’s prescription, physicians should be aware that it may reveal the underlying cardiovascular problem. Thus, physicians must also consider the underlying medical conditions when prescribing sildenafil.
Male erectile dysfunction (ED) is defined as the inability to attain and/or maintain a penile erection sufficient for satisfactory sexual performance. The overall reported ED prevalence rate in South Korea ranges from 8% to 45.8% according to patient demographics [1] and is estimated to affect more than 150 million men globally [2]. Sildenafil citrate is the first oral agent approved for the treatment of ED [3]. Several studies have shown that sildenafil citrate is safe for use in patients with cardiovascular disease as well as in healthy individuals [4, 5, 6, 7, 8, 9]. However, although the occurrence is low, there may be significant cardiovascular accidents. Especially, co-administration of nitrates and sildenafil citrate greatly raises the risk of life-threatening hypotension [10, 11]. Therefore, sildenafil citrate is not recommended for patients with coronary artery disease who are already receiving nitrates.
Herein, we describe a rare case in which a patient with no cardiovascular risk factors except heavy smoking and heavy drinking, who had an ST-segment elevation myocardial infarction (STEMI) after receiving sildenafil citrate.
A 40-year-old man presented to our emergency department with acute chest pain,
diaphoresis, and dyspnea. He had no underlying disease and was not on any
prescription medication: he had no history of hypertension, diabetes mellitus,
dyslipidemia, denied erectile dysfunction, and had no psychiatric illness.
However, he was a heavy current smoker (40 pack-years) and a heavy drinker (1 L
of beer three to four times a week). His height was 175 cm with a weight of 51
kg, a body weight index of 16.7 (kg/m
 Fig. 1.
Fig. 1.The electrocardiogram (ECG) of the patient at the initial visit of the emergency department, complaining chest pain. ST elevations can be seen in the ECG leads of II, III and aVF (A), and the ECG 15 minutes after intravenous hydration of 500 mL of normal saline, where the ST elevations in ECG leads of II, III and aVF have normalized (B).
However, in the morning, although his ECG showed no ST elevation, CK-MB and
troponin-I both increased to 60.6 ng/mL and 2.047 ng/mL, respectively. In
addition, transthoracic echocardiography revealed left ventricular (LV)
dysfunction, with LV ejection fraction of 41% (normal:
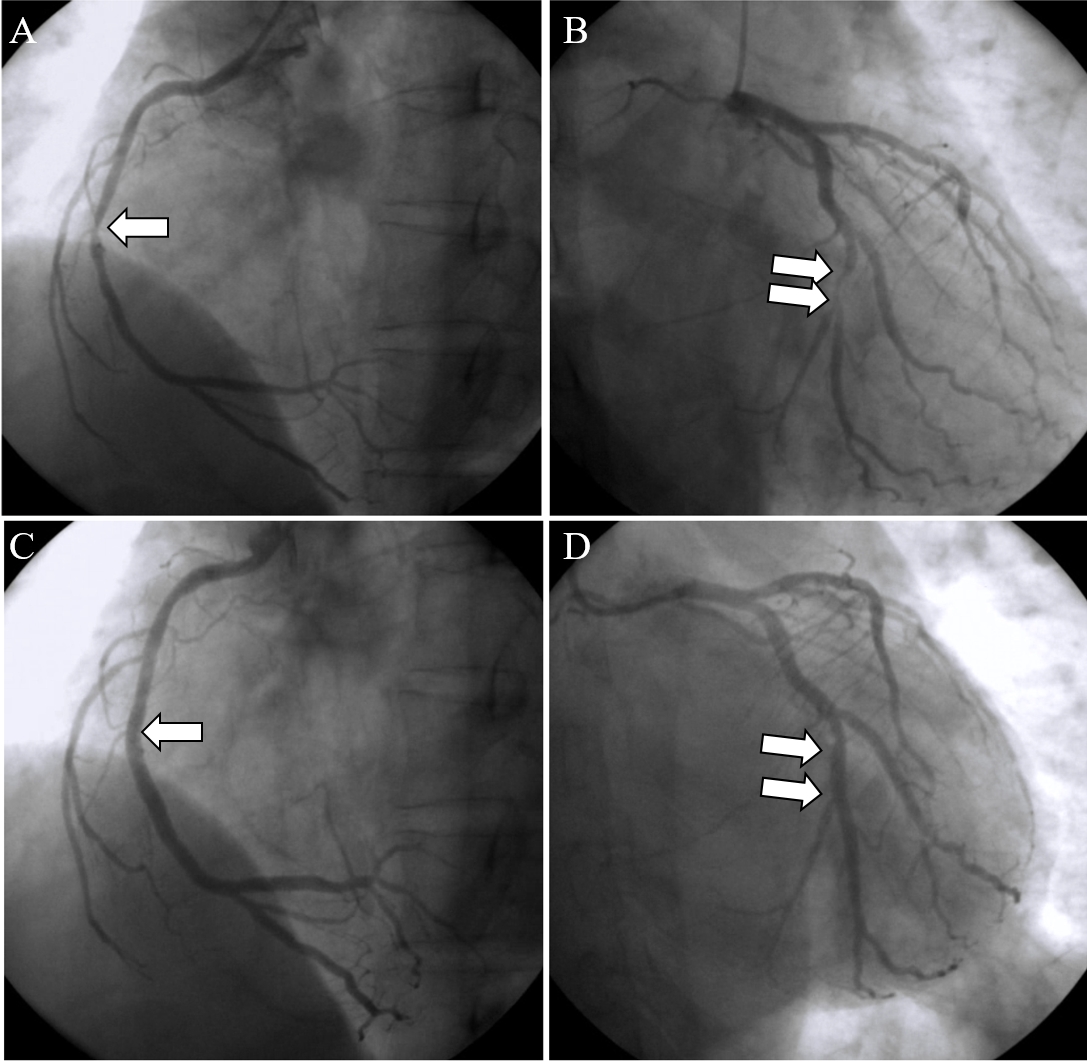 Fig. 2.
Fig. 2.Elective coronary angiogram of the right coronary artery (RCA)
and the left circumflex coronary arteries (LCx). The middle RCA had stenosis of
90%, shown by the white arrow (A), and the distal LCx had focal stenosis of
85%, shown by the white arrows (B). One stage primary coronary intervention
(PCI) on the middle RCA was performed (3.5
A high prevalence and incidence of worldwide ED has been observed in recent epidemiological data and is projected to double by 2025 [2]. In a large survey conducted in Korea, 13.4% of 1,570 men with an age range of 40-79 years suffered from ED [12]. In another Korean study of 3,501 men of age over 20 years, the prevalence of ED who visited primary care physicians was 36.6% [13]. Age, diabetes, hypertension, obesity, lack of exercise, and smoking are risk factors for ED, and as these factors are increasing, sildenafil is also increasing. In addition, we believe the population on sildenafil is higher than the previously reported factors due to its recreational usage.
Sildenafil citrate is the first approved oral phosphodiesterase type 5 inhibitor for the treatment of ED [3]. It selectively inhibits cyclic guanosine monophosphate and induces relaxation of the blood vessels and smooth muscles, which enhances penile erection, with modest reductions in BP, insufficient to stimulate a reflex increase in heart rate. Indeed, sildenafil is not associated with a short-term risk for myocardial infarction (MI). Moreover, studies have reported that sildenafil is not associated with an increased risk of cardiovascular events [7, 8, 9]. Furthermore, there has been no reported hemodynamic interaction between sildenafil and red wine [14]. However, there is conflicting evidence on associations between sildenafil and cardiovascular diseases; vasodilation and hypotension from sildenafil as the cause of the increased the risk of developing MI [15] versus vasodilation improving coronary artery flow reserve from increased hemodynamic flow [16]. Reviews on cardiovascular risk and sildenafil show deaths from cardiovascular diseases are the highest, however, the death rate was slightly higher in the placebo groups than the sildenafil groups arguing the safety of sildenafil [17].
In patients without a prior history of coronary artery disease, sildenafil-associated MI is rarely seen [18, 19]. However, we report a rare case, where the patient consumed sildenafil with alcohol in the attempt of engaging in sexual activity that revealed the underlying coronary disease. Like dipyridamole, which was previously used in non-invasive pharmacological stress tests to diagnose coronary artery disease, we believe that sildenafil expands all coronary arteries, in effect, shifting more blood flow to the left anterior descending (LAD) artery, a non-obstructive coronary artery. Therefore, this may steal blood from the deprived region distal to obstruction and aggravate the ischemia of the obstructive lesion of RCA and LCx. This, without compensating heart rate increase, reduced the total blood flow, which could not meet the demand required by the LAD, revealed the underlying coronary disease, as can be seen in coronary steal syndrome [20]. If the patient had variant angina, sildenafil might not have triggered ST elevation; on the contrary, it may have improved his symptoms of chest pain and dyspnea.
The American College of Cardiology and American Heart Association expert consensus reported an executive summary on the use of sildenafil in patients with cardiovascular diseases [11]. The summary table (Table 1) is reprinted for clarity [11], and based on the table, our patient had no contraindications, such as the use of nitrates or antihypertensives. However, Table 1, in retrospect, shows that our patient might have belonged to the B-1 category. According to this report, we believe that sildenafil can trigger similar MI events in patients with asymptomatic severe stenosis of the coronary artery.
| Summary Table of Clinical Recommendations in the Use of Sildenafil |
| A. Use of sildenafil clearly contraindicated |
| 1. Concurrent use of nitrates |
| B. Cardiovascular effects of sildenafil may be potentially hazardous (use dependent on individual clinical assessment) |
| 1. Patients with active coronary ischemia who are not taking nitrates (e.g., positive exercise test for ischemia) |
| 2. Patients with congestive heart failure and borderline low blood pressure and borderline low volume status |
| 3. Patients on a complicated, multidrug, antihypertensive program |
| 4. Patients taking drugs that can prolong the half-life of sildenafil |
The expenditure of cardiac and metabolism during sexual intercourse depends on the type of sexual activity. Hemodynamic changes related to sexual intercourse can be much greater with an unfamiliar person, an unfamiliar environment, excessive eating and drinking than a familiar partner. In general, people with the highest risk are middle-aged and have an extramarital relationship. Individual variation may be present in cardiovascular response during sexual intercourse from 2.0 to 5.4 metabolic equivalents (METS), which is a wide variation. Thus, equating the level of cardiac or metabolic expenditure during sexual intercourse with activities such as “climbing the first or second floor” can underestimate the level of cardiovascular response for each individual [11]. In previous old studies of “The so-called coition death” [21], sexual activity was only 0.9% likely to be the cause of the onset of myocardial infarction. Taking this all into account, we recommend using the Duke Activity Status Index (DASI, https://www.mdcalc.com/duke-activity-status-index-dasi) to determine the patient’s cardiovascular risk, where patients with less than 5-6 METs exercise capacity should consult a cardiologist [11].
There are limitations of this case report, the first is that plasma sildenafil levels were not measured to corroborate the patient’s sildenafil intake. As the patient was admitted by the emergency department, and since the patient’s status was an acute state, there was no time to check if there were any commercial laboratories that perform plasma sildenafil levels. Additionally, we have tried to seek commercial laboratories measuring plasma sildenafil, however, there were no laboratories measuring plasma sildenafil levels in Korea. Furthermore, the Ministry of Health and Welfare of Korea does not reimburse the cost of plasma sildenafil levels as checking this has no clinical benefit as in treatment antidote.
Another argument that may be made is his pulmonary vasculature might have been impaired which was exacerbated by sildenafil. Groom et al. [22], recommended not to prescribe sildenafil due to fetal growth restriction. However, there is no evidence that sildenafil impairs the lung vasculature in matured adult lungs, let alone in a single sildenafil intake, which was the case in our patient, who denied previous sildenafil intake.
With the current trend of sildenafil becoming a recreational drug widely available without a physician’s prescription, physicians should be aware that sildenafil may reveal the underlying cardiovascular problem. In addition, physicians must consider underlying medical conditions when prescribing sildenafil.
BWY contributed to the diagnoses, data curation, and writing of the manuscript. JH contributed to the conceptualization and reviewed the manuscript. All authors have read and approved the final manuscript.
For publication of this case report and any accompanying photos, the IRB has waived the requirement of informed patient consent of this publication, as there is no potential harm resulting from a breach of confidentiality, and as this will not adversely affect the rights and welfare of the patient. A copy of the IRB (IRB2021-14, Project number EMCS 2021-02-008) is available for review by the Editor-in-Chief of this journal.
The authors declare no acknowledgments.
No funding sources.
The authors declare no conflict of interest.