


 , Imran Qamar 1, Kawser Ahmed 1, Farjana Bilkis 3, Muhammad Sarwar 1
, Imran Qamar 1, Kawser Ahmed 1, Farjana Bilkis 3, Muhammad Sarwar 11 Acute Medicine, Northampton General Hospital, NN1 5BD Northampton, UK
2 Buckinghamshire New University, HP11 2JZ High Wycombe, UK
3 Department of Cardiology, Manikganj Medical College and Hospital, 1800 Manikganj, Bangladesh
Abstract
Orthostatic hypotension (OH) is a frequently undiagnosed condition, particularly affecting older adults and individuals with autonomic dysfunction. This comprehensive review offers a unique synthesis of current evidence on the aetiology, prevalence, diagnosis, and management of OH, integrating perspectives from neurology, cardiology, and geriatric medicine. It critically appraises the current limitations within clinical guidelines, highlighting the lack of standardised diagnostic protocols and the inadequate recognition of delayed OH and postural hypertension. Particular focus is given to the older population, proposing individualised diagnostic and therapeutic strategies to address their specific clinical vulnerabilities. By adopting a multidisciplinary, patient-centred framework, the review addresses the complexity of diagnosing and managing OH, emphasising both underutilised non-pharmacological interventions and the careful use of pharmacological therapies. It also calls for the urgent revision of national guidelines, including those by the National Institute for Health and Care Excellence, to align with contemporary evidence and improve clinical decision-making. Future research directions are proposed, particularly regarding symptomatic versus asymptomatic OH, the development of refined diagnostic tools, and the long-term impact of symptom control.
Keywords
- orthostatic hypotension
- postural hypotension
- syncope
Orthostatic hypotension (OH) is a prevalent yet frequently underdiagnosed condition, particularly affecting older adults and individuals with autonomic dysfunction [1]. It is clinically defined as a sustained decrease in systolic blood pressure of at least 20 mmHg or diastolic blood pressure of at least 10 mmHg within three minutes of standing or following a head-up tilt of at least 60 degrees [1]. OH often presents with symptoms such as dizziness, visual disturbances, syncope, and generalised weakness, and it is associated with an increased risk of falls, cognitive decline, depression, cardiovascular disease, and mortality [2, 3]. According to the National Institute for Health and Care Excellence [4], inpatients aged 65 years and over, as well as those between 50 and 64 years with predisposing conditions, are deemed at high risk for falls and should have their blood pressure measured both in lying and standing positions upon admission. The management of OH in older adults necessitates an individualised approach that prioritises non-pharmacological strategies, careful medication review, and balancing fall risk against blood pressure targets, recognising the vulnerability of this population to both hypotension and adverse drug effects. OH significantly impairs patients’ quality of life, contributing to recurrent falls, loss of independence, reduced functional capacity, and psychological consequences such as fear of falling and depression [5]. From a health economic perspective, OH is associated with increased healthcare resource utilisation, including higher rates of hospital admissions, emergency department attendances, and prolonged inpatient stays, particularly among older adults [6]. The cumulative burden of OH on healthcare systems underscores the urgent need for improved recognition, standardised diagnostic pathways, and evidence-based management strategies aimed at reducing morbidity, mortality, and associated costs.
Despite its significant clinical consequences, the diagnosis and management of OH are constrained by inconsistent screening practices, outdated national guidelines, and variability in therapeutic approaches. Existing reviews often address singular aspects of OH; however, this review uniquely integrates evidence from neurology, cardiology, and geriatric medicine, offering a comprehensive multidisciplinary perspective. It critically examines the limitations within current practice, emphasises the need to recognise delayed OH and postural hypertension, and advocates for a patient-centred, evidence-based management strategy. Given the increasing burden of OH in ageing populations and its association with significant morbidity and mortality, a standardised and updated approach to its diagnosis and treatment is urgently required. The following section discusses the epidemiology of OH.
The prevalence of OH increases with age, though it varies depending on underlying medical conditions and population characteristics. Systematic reviews estimate that OH affects 19% to 22% of community-dwelling adults, but this figure fluctuates based on study cohorts [7, 8]. Large-scale population studies in the USA indicate a prevalence of less than 5% in individuals under 54 years of age, rising to approximately 14% among those aged 65–69 years and exceeding 20% in individuals aged 80 years and older [9].
A systematic review and meta-analysis of 26 studies involving over 25,000
participants further examined the prevalence of OH in older adults [8]. This study included individuals aged 60 years and older from both
community and long-term care settings. OH was found in 22.2% of
community-dwelling adults and 23.9% of those in long-term care facilities.
However, significant heterogeneity (I2
OH is particularly prevalent among individuals with neurodegenerative disorders. Approximately one-third of patients with Parkinson’s disease are affected by OH, largely due to autonomic dysfunction associated with neurodegeneration [10].
Among institutionalised older adults, the prevalence is notably higher, affecting 31% to 37% of nursing home residents and reaching 68% in geriatric inpatients [7, 11, 12]. Cremer et al. [13] further highlighted that OH is common among geriatric inpatients, with its prevalence influenced by factors such as clinical settings, mobilisation efforts, and the frequency of blood pressure assessments. The increased prevalence in care settings is likely due to the cumulative burden of risk factors, including neurodegenerative disorders, polypharmacy (e.g., antihypertensives, antidepressants), and reduced physical activity leading to deconditioning. Given its strong association with frailty, OH represents a significant clinical concern in older populations, necessitating early detection and appropriate management to mitigate its impact on morbidity and quality of life.
Ageing is inherently linked to a decline in autonomic buffering capacity, which compromises the physiological adaptation to orthostatic stress [14]. This predisposes older individuals to OH, a condition exacerbated by various pharmacological agents, including alpha-blockers prescribed for benign prostatic hypertrophy, central sympatholytic medications such as tizanidine and methyldopa, tricyclic antidepressants, phosphodiesterase-5 inhibitors for erectile dysfunction, and a range of antihypertensive agents, including beta-blockers [15]. Additionally, vascular stiffening due to atherosclerosis, physical deconditioning, and hypertension contribute to impaired compensatory mechanisms, increasing susceptibility to OH [7].
Neurogenic OH arises due to autonomic dysfunction, frequently occurring in conditions such as diabetes mellitus and amyloidosis, where peripheral neuropathy leads to autonomic impairment [16]. Furthermore, neurodegenerative disorders, including Parkinson’s disease and dementia with Lewy bodies, are commonly associated with autonomic dysfunction, resulting in OH of varying severity [17]. Less prevalent but clinically significant disorders affecting the autonomic nervous system include pure autonomic failure, a synucleinopathy primarily affecting peripheral autonomic nerves without concurrent movement disorder, and multiple system atrophy (MSA), which presents with either parkinsonian (MSA-P) or cerebellar (MSA-C) phenotypes, both exhibiting severe autonomic failure, including OH.
Autoimmune autonomic ganglionopathy represents another potential cause of autonomic failure and OH, often characterised by the presence of antibodies targeting the nicotinic acetylcholine receptor at autonomic ganglia. Additionally, paraneoplastic syndromes, most notably those associated with small-cell lung cancer, monoclonal gammopathies, or light-chain diseases, can result in autonomic dysfunction, manifesting as OH. Given the diverse aetiological spectrum, a thorough assessment is essential to distinguish neurogenic from non-neurogenic causes, ensuring accurate diagnosis and targeted management of OH.
Non-neurogenic causes are more prevalent and involve multiple physiological disruptions. Volume depletion, resulting from dehydration, haemorrhage, or hyperglycaemia, significantly contributes to OH. Cardiovascular diseases, including aortic stenosis, heart failure, and arrhythmias, can impair circulatory responses to postural changes. In addition, adrenal insufficiency, prolonged immobilisation, and physical deconditioning further increase the risk. In addition, peripheral neuropathies, often secondary to conditions such as diabetes mellitus, vitamin B12 deficiency, renal failure, amyloidosis, and autoimmune or paraneoplastic syndromes, can lead to autonomic dysfunction, further increasing susceptibility to OH. A systematic review and meta-analysis encompassing 21 studies with 13,722 patients found that approximately 25% of individuals with diabetes experience OH [18]. High glycated haemoglobin (HbA1c) levels, hypertension, and diabetic neuropathy significantly increase the risk [19].
Pharmacological agents play a major role in OH by reducing blood volume or interfering with autonomic regulation [20]. These include antihypertensives (Table 1, Ref. [21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31]), selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants (TCAs), antipsychotics, and beta-blockers. Rather than a single drug class being primarily responsible, evidence suggests that the cumulative number of antihypertensive medications prescribed is a stronger predictor of OH [3]. Individual susceptibility varies based on age, comorbidities, and polypharmacy. Moreover, a recent meta-analysis of randomised controlled trials presents additional evidence that medications inducing sympathetic inhibition are significantly linked to an increased likelihood of OH. In contrast, drugs that primarily exert vasodilatory effects do not demonstrate a similar association [21].
| Antihypertensive class | Association with OH | Study findings |
| Alpha-blockers (e.g., Doxazosin, Prazosin) | Strongly associated with OH due to interference with sympathetic compensatory mechanisms, leading to vasodilation and reduced vascular resistance. | Studies found a higher incidence of OH among patients taking alpha-blockers compared to other antihypertensive classes, leading to increased dizziness and falls [22, 23]. |
| Beta-blockers (e.g., Metoprolol, Atenolol, Propranolol) | Strongly associated with OH due to inhibition of sympathetic responses, reducing heart rate and cardiac output. | A recent meta-analysis of randomised trials provides further evidence that drugs causing sympathetic inhibition are associated with a significantly increased odds of OH, whereas medications with a predominantly vasodilator mechanism of action are not associated with OH [21]. |
| Central sympatholytics (e.g., clonidine, methyldopa) | Strongly associated with OH due to central inhibition of sympathetic outflow, leading to reduced vascular tone and BP variability. | Clonidine, an alpha-2 agonist, decreases sympathetic tone and plasma norepinephrine levels. The review notes that while the effects of clonidine on orthostatic blood pressure have been inadequately investigated, its reduction of sympathetic activity may impair adrenergic compensatory responses to standing, potentially promoting OH [23]. |
| Godbole and Aggarwal [24] found that while clonidine typically lowers blood pressure via central alpha-2 agonism, in patients with autonomic failure, it may instead act on post-synaptic venous alpha-2 adrenoreceptors, promoting venoconstriction and stabilising blood pressure. This paradoxical effect suggests that clonidine’s impact on OH depends on individual autonomic function, necessitating careful patient selection and monitoring. | ||
| Dihydropyridine calcium channel blockers (e.g., amlodipine, nifedipine) | Generally, not associated with OH, but some studies report exceptions where postural BP reductions were observed. | A secondary analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) found that amlodipine was not associated with a higher risk of diagnostic codes for OH compared with lisinopril or chlorthalidone. However, it was associated with a higher risk of falls in the short term. This suggests that while amlodipine may not directly cause OH, it could contribute to fall risk shortly after initiation [25]. |
| ACE inhibitors (e.g., lisinopril, ramipril, enalapril) | Neutral or protective effect against OH, as ACE inhibitors primarily act on the renin-angiotensin system rather than sympathetic tone. | Among ACE inhibitors, the risk of OH appears to vary between specific agents. For instance, enalapril and captopril have been associated with a higher risk of OH, whereas perindopril has demonstrated a lower incidence of hypotension [23]. |
| Angiotensin receptor blockers (ARBs) (e.g., losartan, valsartan) | Neutral or protective effect against OH, with studies showing minimal impact on postural blood pressure regulation. | A cross-sectional analysis of the SPRINT trial found that greater postural reductions in SBP were associated with calcium channel blockers as well as alpha and beta-blockers, but it did not differentiate between dihydropyridine and non-dihydropyridine calcium channel blockers [26]. |
| Diuretics (general) (e.g., hydrochlorothiazide, indapamide) | Associated with OH, particularly in older adults, in whom diuretics may cause volume depletion and electrolyte imbalances. | An observational study has found that diuretics and, in particular, loop diuretics, are associated with OH, with an increased risk of falls and dizziness in older adults [27]. |
| Loop diuretics (e.g., furosemide, bumetanide) | Strongly associated with OH due to excessive fluid loss, electrolyte imbalance, and intravascular volume depletion [26]. | A case cross-over study of over 90,000 adults aged |
| Chlorthalidone | Not clearly linked to increased OH risk compared to other diuretics [29]. | A recent review by Raber et al. [29] found that chlorthalidone did not significantly increase OH risk when compared to other diuretics. |
| Non-dihydropyridine calcium channel blockers (e.g., verapamil, diltiazem) | Potentially associated with OH, though differentiation between dihydropyridine and non-dihydropyridine calcium channel blockers is lacking in many studies. | The SPRINT trial suggested a possible association between non-dihydropyridine calcium channel blockers and greater postural reductions in BP, though the effect size was not substantial [30]. |
| Amlodipine | Short-term increased risk of falls observed in studies. | A randomised controlled trial indicated that amlodipine may elevate the risk of falls during the initial year of treatment. Specifically, compared to chlorthalidone, amlodipine was associated with a hazard ratio of 2.24 (95% CI: 1.06–4.74; p = 0.03), and when compared to lisinopril, the hazard ratio was 2.61 (95% CI: 1.03–6.72; p = 0.04) [31]. |
OH, orthostatic hypotension; CI, confidence interval; BP, blood pressure; ACE, angiotensin-converting enzyme; SBP, systolic blood pressure; SPRINT, Systolic Blood Pressure Intervention Trial.
Hypertension is paradoxically associated with OH due to mechanisms such as reduced diastolic filling, arterial stiffness, and an exaggerated threshold effect in individuals with high supine or seated blood pressure [7]. This impaired baroreceptor sensitivity hinders the compensatory responses required to maintain blood pressure upon standing, increasing the likelihood of OH episodes.
Alcohol consumption contributes to OH through both acute and chronic mechanisms [32]. Short-term effects include vasodilation and impaired vasoconstriction, leading to transient OH. Chronic alcohol use, due to its neurotoxic effects, results in autonomic dysfunction, making it a potential neurogenic cause of OH.
In some cases, OH occurs without a clearly identifiable cause, termed idiopathic OH [33]. This remains a diagnostic challenge, necessitating comprehensive evaluation to rule out secondary causes and optimise management strategies.
A thorough history and clinical examination are essential in assessing patients with suspected OH to determine underlying causes, which are often multifactorial. The history should focus on the nature, onset, and triggers of symptoms, while the examination aims to identify associated autonomic dysfunction, neurological abnormalities, and cardiovascular pathology.
A holistic history is crucial for identifying OH, as patients commonly report light-headedness, dizziness, visual disturbances (tunnel vision or blackouts), and generalised weakness [4]. Symptoms should be assessed in relation to changes in posture, worsening on standing, and improvement upon sitting or lying down [34]. Some patients, particularly those with cognitive impairment, may struggle to articulate their symptoms and instead present with unexplained falls or transient episodes of unresponsiveness. Aggravating factors such as prolonged standing, early morning hours, postprandial states, hot environments, or recent physical exertion should be explored, as these can exacerbate OH due to reduced circulatory compensation [3].
A history of neuropathy should be sought, as small-fibre peripheral neuropathies affecting the lower extremities may indicate underlying autonomic dysfunction [35]. Patients may report symptoms such as burning pain, tingling, or numbness, commonly associated with diabetes mellitus but also seen in conditions such as amyloidosis, autoimmune disorders, or chronic kidney disease. A subacute or acute onset of severe, disabling OH may suggest an autoimmune autonomic ganglionopathy, particularly if preceded by a viral-like illness [3]. In some cases, OH may be a manifestation of a paraneoplastic syndrome, warranting a thorough review of symptoms such as unexplained weight loss or malignancy-associated conditions [36].
Medication history is a key component of the assessment, as OH can be drug-induced [20]. Agents such as alpha-blockers, beta-blockers, nitrates, diuretics, antidepressants, and antipsychotics can impair autonomic responses or reduce intravascular volume, increasing susceptibility to OH. Polypharmacy and recent medication adjustments should also be reviewed, particularly in elderly patients.
The physical examination should focus on confirming the diagnosis of OH and
identifying any underlying neurological or cardiovascular abnormalities. Blood
pressure and heart rate should be measured in both supine and standing positions,
with a drop in systolic blood pressure of
Neurological examination is crucial, as features such as bradykinesia, rigidity, resting tremor, and hypomimia may indicate Parkinson’s disease or multiple system atrophy, both of which are associated with autonomic dysfunction. Cerebellar signs, including ataxia of gait and dysarthria, may suggest multiple system atrophy with predominant cerebellar involvement. In addition, autonomic features such as reduced or excessive sweating, heat intolerance, dry skin, or focal hyperhidrosis may indicate a primary autonomic failure.
Cardiovascular assessment should include auscultation for murmurs suggestive of structural heart disease, such as aortic stenosis, which can contribute to OH. The presence of resting tachycardia or impaired heart rate variability may suggest autonomic neuropathy, particularly in patients with diabetes. Symptoms of gastrointestinal dysmotility, including early satiety, constipation, or bloating, should be assessed, as these are frequently seen in patients with autonomic dysfunction and may precede the development of OH in neurodegenerative disorders. Bladder function should also be evaluated, as urinary frequency, urgency, and nocturia are common in patients with autonomic failure. These symptoms can be particularly pronounced in multiple system atrophy and Parkinson’s disease, where nocturnal hypertension contributes to increased overnight urine production, worsening OH symptoms in the morning. Erectile dysfunction and absent ejaculation in male patients may further indicate autonomic involvement.
A comprehensive approach combining history-taking and clinical examination is vital in identifying the underlying cause of OH and guiding appropriate management. Given the often-multifactorial nature of OH, an interdisciplinary approach involving neurology, cardiology, and geriatric medicine may be necessary for optimal patient care.
A systematic approach to diagnosing OH requires a combination of clinical assessment, bedside measurements, and targeted laboratory and autonomic function tests. The aim is to confirm the presence of OH, distinguish between neurogenic and non-neurogenic causes, and identify any underlying conditions contributing to autonomic dysfunction.
The diagnosis of OH is confirmed through a structured blood pressure assessment in different postural positions (Fig. 1, Ref. [37]). According to the Royal College of Physicians [38], blood pressure should be measured after the patient has been lying supine for at least five minutes, followed by a second reading within the first minute of standing, and a third measurement after three minutes of standing. If blood pressure continues to drop, additional recordings may be necessary. Any symptoms experienced during postural change should be documented. A diagnosis of OH is confirmed if there is a systolic blood pressure reduction of 20 mmHg or more upon standing, a systolic pressure drops below 90 mmHg regardless of their symptoms or less than 20 mmHg, or a diastolic pressure drop of 10 mmHg with symptoms, though systolic changes are considered more clinically relevant.
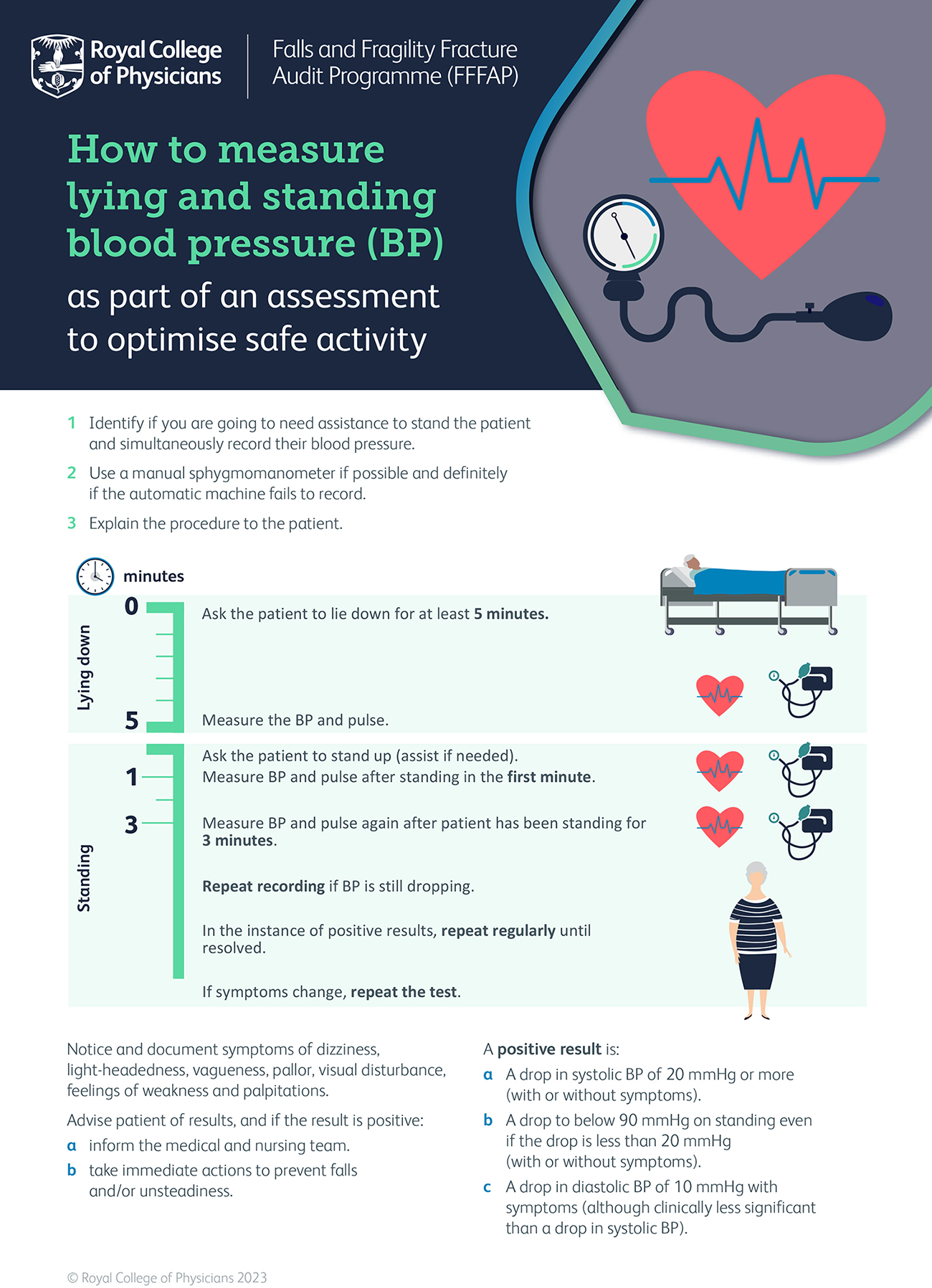 Fig. 1.
Fig. 1.
Measuring orthostatic hypotension. Reproduced from: ‘How to measure lying and standing blood pressure (BP) as part of an assessment to optimise safe activity’. Falls and Fragility Fracture Audit Programme (FFFAP) London: RCP, 2023 [37]. Copyright © 2023 Royal College of Physicians. Reproduced with permission.
It is also advisable to record heart rate responses, as a rise of
| Category | Test name | Purpose | Clinical relevance |
| Autonomic function testing | Deep Breathing Test [39] | Evaluates heart rate variability with respiration. Reduced variation suggests autonomic dysfunction. | Helps assess autonomic dysfunction severity and progression. |
| Valsalva Manoeuvre [39] | Assesses baroreflex function by measuring heart rate and blood pressure responses to forced expiration against resistance. A blunted response suggests autonomic failure. | Essential for diagnosing baroreflex failure and autonomic neuropathies. | |
| Head-Up Tilt-Table Testing [39] | Used when orthostatic vital signs are inconclusive or for differentiating OH from vasovagal syncope. | Key test for differentiating between autonomic and neurally mediated hypotension. | |
| Biochemical investigations | Plasma Noradrenaline Levels [40] | Distinguishes between pre-ganglionic and post-ganglionic autonomic dysfunction. Levels should double upon standing; failure indicates autonomic failure. | Distinguishes between different causes of autonomic failure. |
| Serum and Urine Protein Electrophoresis [41] | Screens for monoclonal gammopathy and light-chain disease, which may contribute to autonomic dysfunction. | Useful for detecting plasma abnormalities linked to autonomic neuropathy. | |
| Random cortisol and short Synacthen test [42] | Random cortisol measurement and the short Synacthen test are used to assess adrenal function when adrenal insufficiency is suspected in OH patients. | These tests help determine cortisol deficiency, which can contribute to OH by impairing vascular tone and sodium retention. | |
| Neurophysiological investigations | Nerve Conduction Studies (NCS) & Electromyography (EMG) [43] | Identifies peripheral neuropathy, particularly in diabetic or amyloid-related autonomic neuropathy. | Detects large-fibre neuropathy, complementing autonomic function tests. |
| Quantitative Sudomotor Axon Reflex Testing (QSART) [44] | Detects small-fibre neuropathies not visible on conventional NCS, providing additional diagnostic clarity. | Superior for identifying small-fibre autonomic neuropathies. | |
| Specialist investigations | Autoimmune Panel [44] | Tests for nicotinic acetylcholine receptor antibodies in suspected autoimmune autonomic ganglionopathy. | Crucial for diagnosing autoimmune autonomic disorders. |
| Paraneoplastic Screening [44] | Identifies paraneoplastic OH by detecting antibodies (anti-Hu, anti-Yo, anti-Ri, anti-amphiphysin, anti-CV2, anti-Ma2). | Aids in early detection of malignancy-associated autonomic dysfunction. | |
| Fat Aspirate or Biopsy [44] | Confirms systemic amyloid deposits if amyloidosis is suspected. | Key test for diagnosing amyloidosis-related autonomic failure. | |
| Genetic Testing | Identifies hereditary neuropathy, such as transthyretin familial amyloid polyneuropathy. | Important in hereditary autonomic neuropathy evaluation. | |
| Autonomic Antibody Testing [44] | Evaluates the presence of antibodies linked to autonomic neuropathies, helping diagnose immune-mediated autonomic failure. | Supports immune-mediated autonomic failure diagnosis. | |
| Imaging | Chest CT [44] | Detects small-cell lung cancer, the malignancy most commonly associated with paraneoplastic OH. | Essential for detecting underlying malignancies causing secondary OH. |
BMJ, British Medical Journal; CT, computed tomography.
Current guidelines for detecting OH vary in definitions, measurement protocols,
and limitations (Table 3, Ref. [37, 45, 46, 47, 48, 49, 50]). While most define OH as a fall in systolic blood
pressure (SBP)
| Guideline/Source | Definition of postural hypotension (PH) | Measurement protocol | Limitations |
| NICE – Hypertension in Adults: Diagnosis and Management [45] | A fall in SBP of |
Measure BP in the supine or seated position; repeat after standing for at least one minute. | The option to measure initial BP in either the supine or seated position may lead to inconsistent assessments, potentially missing cases of OH. |
| NICE – Postural Hypotension in Adults: Fludrocortisone [46] | A fall in SBP of |
Measure BP after standing for up to three minutes. | Lack of a standardised initial measurement position (supine or seated) may affect the accuracy of PH detection. |
| Royal College of Physicians [37] | A fall in SBP of |
Measure BP after lying for at least five minutes; repeat after standing for one minute and again after three minutes. | Multiple BP measurements may be difficult to perform in high-demand clinical settings. Does not explicitly require symptom documentation alongside BP changes, as it could be positive without any symptoms. |
| American College of Cardiology/American Heart Association [47] | A fall in SBP of |
Measure BP after the patient has been seated and relaxed for over five minutes; repeat immediately and after one to two minutes of standing. | Immediate standing measurements may not capture delayed OH, potentially leading to underdiagnosis. |
| European Society of Hypertension/European Society of Cardiology [48] | A fall in SBP of |
Measure BP in the seated position after five minutes; repeat after standing for one and three minutes. | Initial seated measurements may underestimate OH prevalence compared to supine measurements. |
| Hypertension Canada [49] | Not specified | Measure baseline BP in seated position after five minutes (three readings, discard first and average last two). Measure standing BP two minutes after standing and when symptoms occur. | Lack of a specific OH threshold makes diagnosis less standardised. |
| National Heart Foundation of Australia [50] | Not specified | Measure baseline BP after sitting for several minutes (three readings, average last two). Measure BP once after standing for at least two minutes. | Single standing measurements may fail to detect transient BP drops. |
DBP, diastolic blood pressure; BP, blood pressure.
Current guidelines recommend targeted screening rather than routine population-wide testing. The NICE [4] suggests measuring postural blood pressure in symptomatic patients or those who have experienced a fall. Screening is also advised for patients with hypertension and type 2 diabetes or those over the age of 80 with hypertension.
The American Diabetes Association recommends periodic OH assessment in patients with diabetes, even if asymptomatic. In addition, expert consensus suggests screening individuals diagnosed with neurodegenerative conditions associated with autonomic dysfunction (e.g., Parkinson’s disease, multiple system atrophy) and those with peripheral neuropathies known to affect autonomic function, such as diabetic neuropathy.
Table 4 (Ref. [51, 52]) [3, 4, 26] outlines the differential diagnosis that healthcare professionals should consider when approaching a patient with OH.
| Condition | Description | Key diagnostic features |
| Vasovagal syncope | A common cause of transient loss of consciousness due to reflex bradycardia and vasodilation, often triggered by stress, pain, or prolonged standing. | Triggered by emotional/physical stress, prodromal symptoms (nausea, sweating, pallor), transient loss of consciousness. |
| Reflex tachycardia | A compensatory mechanism where the heart rate increases in response to low blood pressure, sometimes mimicking OH. | Rapid heart rate increases in response to hypotension, often secondary to dehydration or autonomic dysfunction. |
| Postural orthostatic tachycardia syndrome (POTS) | A disorder of autonomic regulation causing excessive heart rate to increase upon standing, often accompanied by dizziness and fatigue. | Excessive heart rate increase ( |
| Carotid sinus syndrome | Hypersensitivity of the carotid sinus leading to syncope, near-syncope, or unexplained falls, particularly in older adults. | Syncope or near-syncope, hypersensitive carotid sinus, tilt-table test may confirm. |
| Postprandial hypotension | Significant drop in blood pressure following meals due to impaired vasoconstriction and autonomic dysfunction. | Blood pressure drops after meals, autonomic dysfunction. |
| Autonomic failure syndromes and neurodegenerative diseases | Includes conditions such as Parkinson’s disease and multiple system atrophy, leading to progressive autonomic dysfunction that mimics OH. | Presence of neurodegenerative disease, progressive autonomic dysfunction. |
| Cardiovascular disorders | Includes arrhythmias, aortic stenosis, and heart failure, which may contribute to orthostatic symptoms. | Cardiac abnormalities, ECG/echocardiogram findings, history of cardiovascular disease. |
| Anaemia | Reduced oxygen-carrying capacity leading to fatigue, dizziness, and exacerbation of orthostatic symptoms. | Low haemoglobin levels, pallor, fatigue, and reduced oxygen delivery. |
| Adrenal insufficiency | Deficiency in adrenal hormones causing hypotension, fatigue, and electrolyte imbalances. | Low cortisol levels, fatigue, salt craving, hypotension. |
| Cardiac arrhythmia | Irregular heart rhythms that may lead to episodic dizziness, palpitations, and syncope. Cardiac pseudo-syncope and postural orthostatic tachycardia syndrome (POTS) [51]. | ECG changes, palpitations, episodic dizziness, syncope. |
| Congestive heart failure | Failure of the heart to pump effectively, resulting in reduced blood flow and orthostatic intolerance. | Peripheral oedema, reduced ejection fraction, exertional dyspnoea. |
| Diabetes insipidus | Impaired kidney function leading to excessive urination, dehydration, and subsequent hypotension. | Polyuria, polydipsia, dehydration signs, hypernatremia. |
| Hyperglycaemia | Elevated blood glucose levels affecting vascular function and autonomic stability. | Fasting blood glucose elevation, polyuria, polydipsia. |
| Hypokalaemia | Low potassium levels causing muscle weakness, arrhythmias, and blood pressure instability. | Serum potassium |
| Myocardial infarction | Ischemic damage to heart muscle potentially leading to autonomic instability and hypotension. | ECG abnormalities, cardiac enzyme elevation, chest pain history. |
| Myocarditis | Inflammation of the myocardium, which can impair cardiac output and result in hypotensive episodes. | Elevated inflammatory markers, ECG and cardiac MRI changes. |
| Pheochromocytoma | A catecholamine-secreting tumour causing episodic hypertension, palpitations, and OH due to autonomic dysfunction. | Paroxysmal hypertension, episodic headaches, sweating, palpitations, abnormal catecholamine levels. |
| Inner ear disease (BPPV) | BPPV is a peripheral vestibular disorder characterised by brief episodes of vertigo triggered by changes in head position relative to gravity. | The Dix–Hallpike manoeuvre is the key diagnostic test, provoking characteristic positional nystagmus with a brief latency, limited duration, and fatigability [52]. |
ECG, electrocardiogram; BPPV, Benign Paroxysmal Positional Vertigo; MRI, Magnetic Resonance Imaging.
The management of OH primarily focuses on alleviating symptoms and preventing complications such as falls and syncope [4]. Treatment is generally reserved for symptomatic patients, as the clinical significance of asymptomatic OH remains uncertain. A multifaceted approach is required, encompassing identification and reversal of underlying causes, patient education, non-pharmacological strategies, and pharmacological interventions when necessary.
A key aspect of OH management involves identifying and addressing modifiable contributors. Medication review is essential, as many commonly prescribed drugs, such as antihypertensives, diuretics, tricyclic antidepressants, and alpha-blockers, can contribute to OH. If a drug-induced cause is suspected, adjustments should be made by either discontinuing, reducing the dose, switching to a modified-release preparation, or substituting with an alternative agent. Care should be taken to ensure that the underlying condition for which the medication was prescribed remains adequately managed.
Other reversible factors include dehydration, infection, anaemia, and electrolyte imbalances, all of which should be corrected where possible. Further investigations should be guided by the patient’s clinical presentation. Blood tests (e.g., full blood count, electrolytes, renal function, HbA1c, vitamin B12 levels) may be warranted to rule out systemic contributors such as diabetes, renal impairment, or vitamin deficiencies. If arrhythmias or structural heart disease are suspected, an electrocardiogram (ECG) and echocardiogram may be appropriate. Furthermore, a referral to falls clinic/syncope or memory clinic might be required as well.
Non-pharmacological interventions are essential in the management of OH, particularly in patients where pharmacological therapy is contraindicated or insufficient. Patient education is central to self-management. Individuals should be informed about the pathophysiology of OH, common exacerbating factors, and preventive strategies. They should avoid prolonged standing, sudden postural changes, large meals, alcohol consumption, dehydration, and exposure to excessive heat. Hot showers and straining should similarly be minimised, as these contribute to vasodilation and intravascular volume depletion, thereby worsening symptoms.
Physical counter-manoeuvres are frequently employed to reduce orthostatic symptoms. Techniques such as leg crossing, squatting, and tensing lower limb muscles before or during standing can augment venous return and limit blood pressure decline. In addition, compression garments—such as abdominal binders or thigh-high stockings—may assist in reducing venous pooling, although their practicality may be limited by discomfort or difficulties in application [53].
Optimisation of hydration status is recommended, including maintaining sufficient fluid intake and, where not contraindicated (e.g., in hypertension or heart failure), increasing dietary salt to expand plasma volume [26]. Postural changes should be performed gradually to allow compensatory autonomic responses to occur. Elevating the head of the bed by approximately 30 degrees can help to reduce nocturnal supine hypertension, which is commonly associated with autonomic dysfunction in OH [26].
Further strategies include leg elevation and active counter-manoeuvres to diminish peripheral venous pooling [26]. Postprandial hypotension, which contributes to symptom burden in many patients, can be addressed by reducing meal size, increasing meal frequency, and limiting carbohydrate-rich foods to prevent splanchnic vasodilation [26]. While compression stockings are often proposed to improve venous return, current evidence supporting their effectiveness is limited. Comparatively, abdominal compression has demonstrated greater efficacy in reducing splanchnic pooling; however, its routine use may be hindered by issues of comfort and patient adherence [53].
When non-pharmacological interventions fail to adequately control the symptoms of OH, pharmacological treatments may be considered. Midodrine, an alpha-adrenergic agonist, is often the first-line therapy; it induces vasoconstriction, thereby increasing standing blood pressure. It is typically initiated at 2.5 mg three times daily during waking hours and may be titrated by increments of 2.5 mg every three to seven days, up to a maximum of 10 mg three times daily [54]. Common adverse effects include supine hypertension, piloerection, pruritus, and urinary retention; therefore, blood pressure should be monitored in both supine and standing positions, and patients should be advised to avoid lying flat shortly after dosing.
Fludrocortisone, a mineralocorticoid, enhances sodium retention and expands plasma volume, contributing to improved blood pressure stability. It is initiated at a dose of 100 micrograms once daily, with gradual escalation by 50–100 micrograms as needed, not exceeding 300 micrograms daily [55]. Monitoring should include blood pressure, serum electrolytes, and fluid status, as fludrocortisone may precipitate fluid overload, hypertension, hypokalaemia, and, in some cases, heart failure.
Other pharmacological options include droxidopa, a norepinephrine precursor that augments sympathetic tone, initiated at 100 mg three times daily, with titration by 100 mg every 24–48 hours to a maximum of 600 mg three times daily, while monitoring for supine hypertension, headache, and nausea [3]. Pyridostigmine, a cholinesterase inhibitor that enhances autonomic function, is often reserved for milder cases and may be commenced at 30–60 mg twice daily, with gastrointestinal side effects such as diarrhoea and abdominal cramps being the most common limitations to its use. In refractory cases, a combination of these agents may be required under specialist supervision to achieve optimal symptom control.
OH has significant clinical implications, affecting both functional ability and long-term health outcomes. It can impair balance and mobility, thereby increasing the risk of falls and reducing the ability to perform activities of daily living. The impact of OH extends beyond transient symptoms of dizziness or syncope, as it is strongly linked to cardiovascular disease, cerebrovascular events, cognitive decline, and increased mortality.
Individuals with OH are at a markedly higher risk of falls, with studies indicating an approximately 1.73-fold increased likelihood compared to those without OH. This is particularly concerning in older adults, where falls can lead to fractures, hospitalisation, and loss of independence.
OH has been associated with a greater incidence of heart failure, with a hazard ratio of 1.34, highlighting the potential role of haemodynamic instability in worsening cardiac function in experimental laboratory research [56]. The risk of coronary heart disease is also elevated (hazard ratio 1.44), suggesting that recurrent episodes of cerebral and myocardial hypoperfusion may contribute to vascular damage and ischaemic events.
Cerebrovascular complications are another major concern, with OH linked to a 1.64-fold increased risk of stroke, possibly due to inadequate cerebral perfusion during hypotensive episodes. The association with atrial fibrillation (hazard ratio 1.51) further highlights the complex cardiovascular consequences of OH, as impaired autonomic regulation and blood pressure fluctuations may predispose individuals to arrhythmias [56]. These cardiovascular risks collectively contribute to a 50% increased risk of all-cause mortality, as demonstrated in a meta-analysis of large-scale prospective observational studies [57]. Emerging evidence from smaller studies suggests that OH may also have detrimental effects on cognitive function, increasing the risk of dementia and cognitive impairment [58, 59]. Chronic cerebral hypoperfusion is thought to play a role in neurodegenerative processes, potentially accelerating cognitive decline. Furthermore, a potential link between OH and depression has been suggested, though the exact mechanisms remain unclear.
The degree to which these risks vary between symptomatic and asymptomatic individuals remains uncertain, as does the influence of age on these outcomes. However, given the broad spectrum of adverse effects associated with OH, early identification and appropriate management are crucial to reducing morbidity and improving quality of life.
Postural hypertension is a phenomenon where blood pressure rises rather than falls upon standing [60]. Unlike OH, which is well-documented and widely recognised, postural hypertension remains under-researched, and its clinical significance is not fully understood. While some definitions classify it as an increase in systolic blood pressure of 20 mmHg or more, variations in study criteria have led to inconsistent prevalence estimates [61]. The mechanisms underlying postural hypertension are not entirely clear, but it is thought to be associated with increased vascular resistance, altered autonomic control, and impaired baroreceptor function. It has been observed in individuals with conditions such as hypertension, diabetes, and neurodegenerative diseases, suggesting a possible link to autonomic dysfunction. In some cases, it may reflect excessive sympathetic activation, while in others, it could indicate vascular stiffness or dysregulated blood pressure responses to positional changes. Emerging evidence suggests that postural hypertension may be linked to an increased risk of cardiovascular events, including heart failure, stroke, and mortality [61]. However, there is ongoing debate about whether it represents a compensatory mechanism or a pathological condition requiring intervention.
It seems that current guidelines, such as NICE, are outdated; therefore, clinical guidelines should be revised to incorporate recent findings on non-pharmacological strategies, symptom prioritisation, and drug-induced hypotension. Future research should not only examine the comparative effectiveness of treatments for classical and delayed OH but also define optimal follow-up strategies for high-risk populations. Patients with underlying neurological conditions, such as Parkinson’s disease or multiple system atrophy, require structured follow-up, including regular assessment of fall history, lying and standing blood pressure measurements, evaluation for supine hypertension, and screening for cardiovascular events. It is advisable that follow-up occurs at intervals of three to six months initially, with more frequent review if new symptoms develop or treatment adjustments are made. Clear follow-up protocols would support earlier identification of clinical deterioration, guide treatment modifications, and ultimately improve long-term outcomes in this vulnerable group.
Effective management of OH requires a comprehensive, multidisciplinary approach that prioritises patient education, lifestyle modifications, and, where necessary, pharmacological interventions. Non-pharmacological strategies, such as maintaining adequate hydration, gradual postural changes, and physical counter-manoeuvres, play a central role, with pharmacological agents such as midodrine and fludrocortisone reserved for more severe or refractory cases. Early recognition and individualised treatment are critical to improving clinical outcomes and reducing complications, particularly in older adults who are at increased risk. The inclusion of postural hypertension in this review reflects the need to recognise the full spectrum of orthostatic blood pressure abnormalities, as postural hypertension may coexist with OH and influence diagnosis, risk stratification, and therapeutic decisions.
Not applicable.
HHA made substantial contributions to the conception and design of the work, conducted the literature review, drafted the manuscript, and contributed to the final critical revision for intellectual content. IQ provided critical review of the manuscript with expert clinical input, provided feedback, contributed to the overall study design and revised the manuscript for important intellectual content. KA, FB, and MS made substantial contributions to data acquisition and critically reviewed the manuscript. All authors approved the final version to be published, and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.