











1 Intestine ClinicOmics Microbiota & Metabolism (InCOMM) Team, French Institute of Metabolic and Cardiovascular Diseases (i2MC), UMR1297 Inserm/Université Toulouse III – Paul Sabatier, 31432 Toulouse, France
2 Service d’Odontologie, Centre Hospitalier Universitaire de Toulouse, 31400 Toulouse, France
3 Département Odontologie, Faculté de Santé de Toulouse, Université de Toulouse, 31400 Toulouse, France
Abstract
Oral health has long been considered to be on the bangs of systemic health. And yet, as recently as 2024, the World Health Organization stated once again that oral diseases rank first in the world in terms of prevalence. This review aims to highlight data from the literature demonstrating the relationships between oral and systemic diseases. The tissues of the oral cavity, teeth, their bony bases and supporting tissues can each suffer from pathologies, often infectious, whose consequences can be found at local, regional and systemic levels. These disorders affect children and adults of all ages. Their management is a public health issue that involves all medical practitioners.
Keywords
- oral health
- dentistry
- cardiovascular diseases
- diabetes mellitus
- microbiota
- infective endocarditis
In recent decades, the scientific community has witnessed a surge of interest in the complex relationships between oral health and systemic diseases [1]. This burgeoning field of research has revealed that the mouth is far more than just a gateway for nutrition; it’s a dynamic ecosystem with considerable implications for general health. The oral cavity hosts a diverse microbiome, home to hundreds of bacterial species that coexist in a delicate balance [2]. This microbial community is as unique as a fingerprint, shaped by factors ranging from diet and lifestyle to genetics and environmental exposures [3]. When in harmony, these microorganisms contribute to oral health and even support broader bodily functions. However, this equilibrium can be easily disrupted. Poor oral hygiene, dietary changes, or compromised immune function can tip the scales, leading to a state of dysbiosis. In this altered state, opportunistic pathogens can flourish, triggering a cascade of events that extend beyond the confines of the mouth. Dental caries and periodontal diseases, once considered isolated oral tissues, are now recognised as potential catalysts for systemic health problems. In the context of dental caries, bacterial species such as Streptococcus mutans (S.m.), Streptococcus sobrinus (S.s.), and various Lactobacillus strains are predominantly found [4]. Conversely, periodontal diseases are characterised by a concomitance of a local immunity dysfunction and the proliferation of different bacterial types [5]. When considering periodontitis, the microbial landscape shifts dramatically, with a predominance of strict anaerobic Gram-negative bacteria. Notable among these are genera from the Fusobacterium, Porphyromonas, and Prevotella families [6]. These anaerobic bacteria thrive in the oxygen-depleted environment of deep periodontal pockets, contributing to the inflammatory processes and tissue destruction associated with periodontal diseases. This distinct microbial profile in caries versus periodontitis underscores the specificity of bacterial involvement in different oral pathologies.
The oral-systemic connection is bidirectional because oral diseases can impact overall health, but systemic conditions can also have manifestations in the oral cavity. This review aims to shed light on the complex mechanisms of oral-systemic interactions, exploring how the health of the human mouth can influence—and be influenced by—the well-being of the entire body. From cardiovascular diseases to diabetes, from respiratory infections to adverse pregnancy outcomes, the implications of oral health are vast and varied. The critical role of oral health in the broader context of human health will be developed, thanks to cutting-edge research and clinical observations.
The human dentition consists of 32 teeth in adults and 20 teeth in children, each specialised for different functions such as cutting, tearing, crushing, and grinding food [7]. The three main tissues of a tooth are the enamel, the hardest substance in the human body [8], the underlying dentin [9] and the soft tissue core, rich in blood vessels and nerves (Fig. 1).
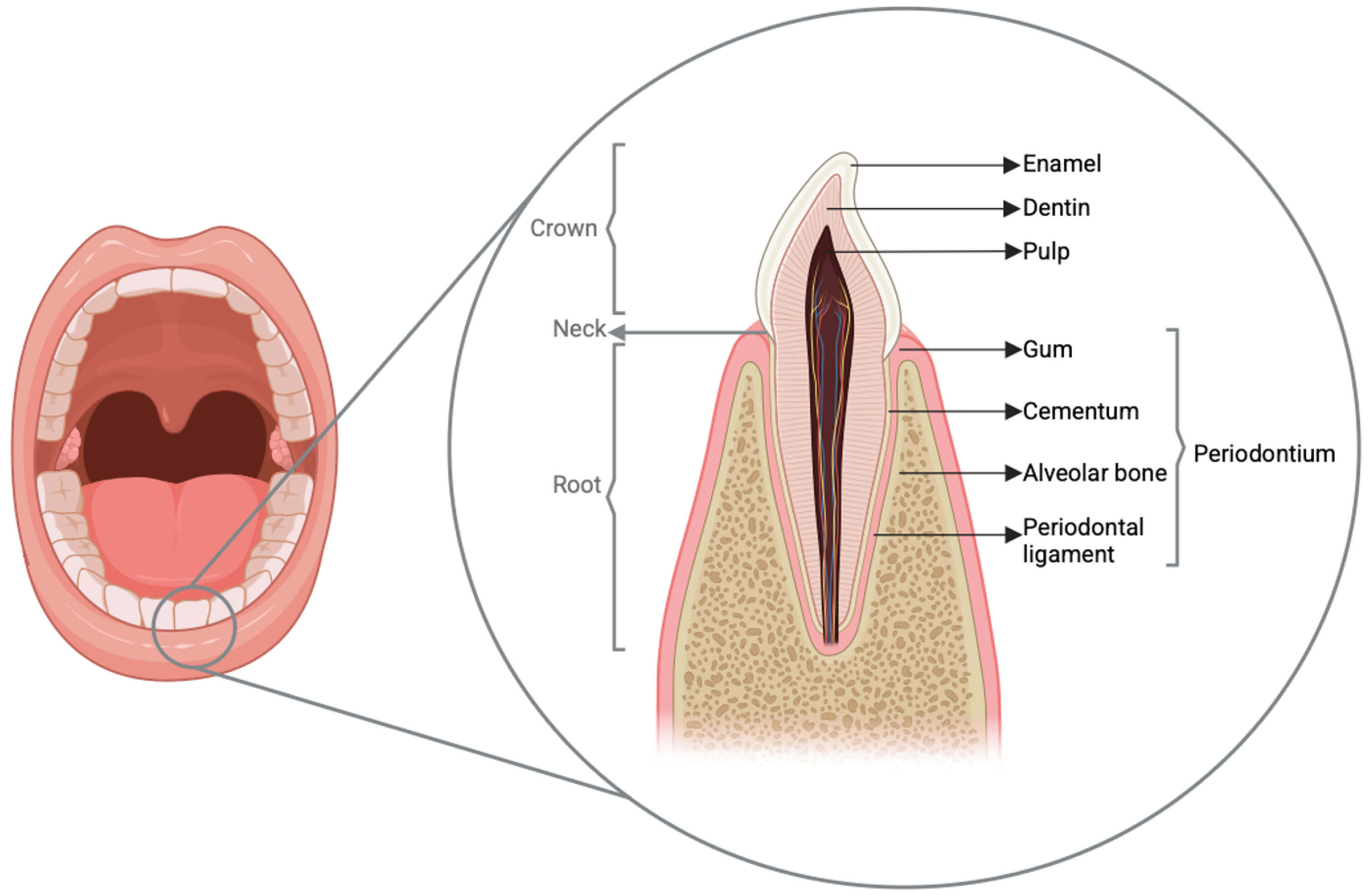 Fig. 1.
Fig. 1.
Schematic overview of dental and periodontal tissues. The enamel is located solely on the crown, whereas cementum is found only on root surfaces. Figure designed with BioRender® (BioRender Inc., Toronto, Ontario, Canada; https://www.biorender.com/).
The periodontium, crucial for tooth anchorage, is composed of four tissues [10]: the gingiva or gum (first line of defense against oral pathogens) [11], the cementum (located on the root surface and displays regenerative properties) [12, 13], the alveolar bone (surrounds dental roots and adapts to masticatory forces) [14] and the periodontal ligament (connects the alveolar bone to the tooth root and acts as a shock absorber) [15].
Understanding these structures and their functions is crucial not only for maintaining oral health but also for appreciating the potential impact of oral conditions on systemic health. The rich vascularisation and innervation of oral tissues, along with their constant exposure to environmental factors, make the oral cavity a potential gateway for systemic effects, highlighting the importance of oral health in overall well-being.
Furthermore, the oral cavity hosts a complex and dynamic microbial ecosystem known as the oral microbiome [16], which plays a significant role in both oral and systemic health and forms biofilms on tooth surfaces and oral mucosa.
Disruptions in the balance of the oral microbiome, known as dysbiosis, can lead to various oral diseases such as dental caries and periodontitis [16]. Moreover, the oral microbiome has been linked to numerous systemic conditions, including cardiovascular diseases, adverse pregnancy outcomes, and respiratory diseases. The potential for oral microbes to influence systemic health underscores the importance of maintaining a healthy oral ecosystem as part of overall health management.
Understanding the composition, dynamics, and interactions of the oral microbiome and biofilms is essential for developing effective preventive strategies and treatments for both oral and systemic diseases [17]. This knowledge reinforces the concept that oral health is an integral component of general health and well-being.
A bacterial biofilm forms continuously in the oral cavity, adhering to the surfaces of teeth and mucous membranes within hours [18]. When oral hygiene is insufficient, the dynamics of oral biofilms lead to dysbiosis, resulting in pathologies in the oral cavity [19].
The silent epidemic of dental decay represents a global health challenge that goes far beyond the simple deterioration of teeth [20]. In November 2024, the World Health Organization published an alarming report in which oral diseases ranked first in diseases worldwide. The international organization also stated that more than 3.5 million people suffered from caries. This disease process results from frequent exposure to carbohydrates, poor oral hygiene, and host factors that promote the production of extracellular polymeric substances (EPS) and organic acids by biofilm bacteria. The environment acidification alters the microbial composition, favouring acidogenic and aciduric bacteria (Streptococcus mutans, Lactobacillus, Actinomyces, Bifidobacterium, Scardovia) while reducing beneficial bacterial diversity [21, 22, 23]. When the pH drops below 5.5, hydroxyapatite crystals found in the enamel begin to demineralise [24], leading to a progressive loss of calcium and phosphate, and a more porous and vulnerable enamel as a consequence.
Initially, patients may only experience some warning signs, but the more the infection penetrates into deeper dental layers and towards the pulp (Fig. 2), the more the body’s inflammatory response intensifies, transforming minor discomfort into significant pain. At this stage, called pulpitis, traditional treatments shift from conservative restoration to more invasive procedures like pulp excision and endodontic therapy [25].
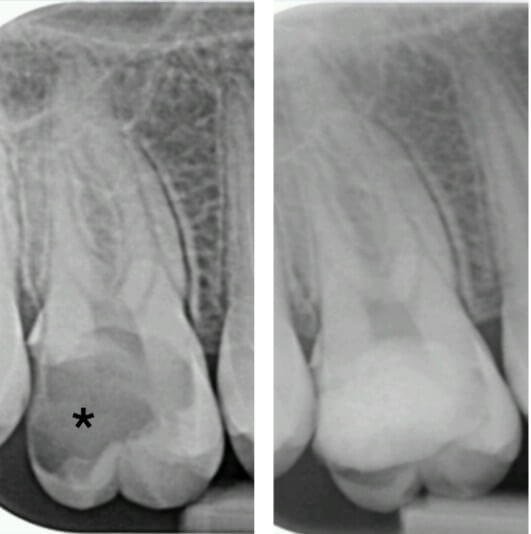 Fig. 2.
Fig. 2.
Intraoral X-ray of tooth #16 before and after carie (*) treatment.
If left untreated, the pulp may become necrotic due to bacterial invasion, potentially resulting in a periapical abscess (Fig. 3). At this point, antibiotic therapy, regularly discussed for misuse in medicine, is often essential alongside surgical interventions such as drainage of the abscess [26]. Once the immediate crisis is addressed, endodontic treatment is necessary to save the affected tooth.
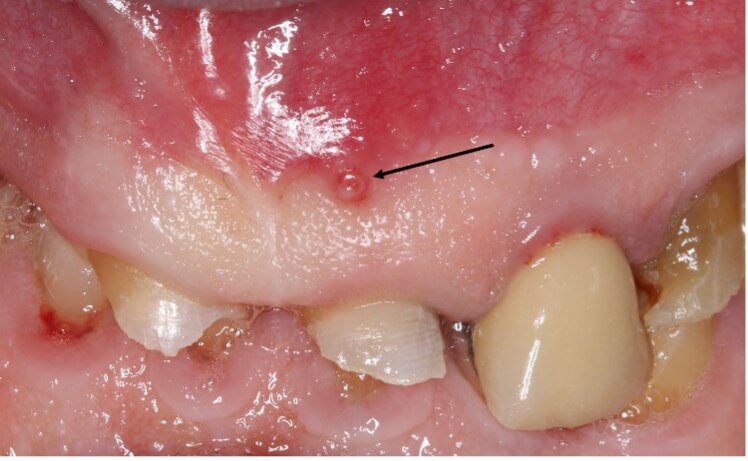 Fig. 3.
Fig. 3.
Photograph of a gingival fistula (arrow) showing the presence of a periapical abscess abutting the tooth.
The implications of periapical infections are not confined to the mouth; they can act as sources for distant infections, including sinusitis related to dental issues [27] (Fig. 4), infections in prosthetic joints [28], or in rare cases, brain abscesses [29]. According to Deppe et al. [30], oral bacteria may be implicated in approximately 10 to 35% of infective endocarditis cases, highlighting a potential link between oral health and cardiovascular conditions.
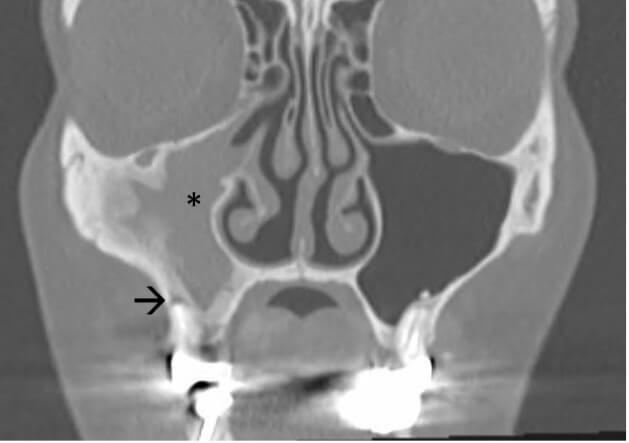 Fig. 4.
Fig. 4.
Computed tomography (CT) scan of a patient with infection of the right maxillary sinus (*) due to chronic apical periodontitis localized on a root (arrow) of tooth #16.
Overall, the potential for oral infections to affect systemic health underscores the importance of timely intervention and preventive care. Regular dental check-ups and prompt treatment of any dental issues are vital for maintaining not just oral but systemic health.
Dental health represents a critical aspect of overall well-being, with prevention strategies extending far beyond simple brushing techniques. The extended presence of certain bacterial species within dental plaque can result in gingival inflammation, commonly known as gingivitis, and superficial damage to the supporting tissues of the tooth. The persistence of dysbiosis in the oral (especially periodontal) microbiome is a significant factor in the onset of deeper periodontal diseases. These conditions arise from an imbalance between pathogenic bacteria and the host’s immune response. As bacteria infiltrate the subgingival area, they contribute to the formation of periodontal pockets and sustain a chronic inflammatory state.
Periodontal diseases as a whole actually include different grades and stages, reflective of a progressive deterioration of the supporting structures of the teeth. In advanced stages, these pathologies can lead to tooth loosening, mobility, and ultimately tooth loss [31, 32]. The classification of periodontal diseases has evolved significantly [33], with recent revisions taking into account the intricate relationships between oral health disturbances and associated systemic conditions [34]. This paradigm shift recognises the periodontal tissues as a mirror of overall patient health [35]. It has been known for nearly 30 years that certain aggressive periodontal conditions, such as necrotising ulcerative gingivitis or periodontitis (Fig. 5), may serve as indicators of underlying severe systemic disorders [36]. These conditions can be early manifestations of serious health issues like leukaemia or acquired immunodeficiency syndrome (AIDS), underscoring the importance of comprehensive health assessment in dental practice [37]. This evolving perspective on periodontal health emphasises the need for interdisciplinary approaches in healthcare. Dental professionals must be vigilant not only while treating local oral conditions but also in recognising potential systemic implications. Conversely, medical practitioners should be aware of the oral manifestations of systemic diseases. Thus, when patient care involves serious pathologies, it is beneficial to coordinate practitioners from all the involved specialities within the same structure, hospital for example [38].
 Fig. 5.
Fig. 5.
Ulcero-necrotic gingivitis in a 30-year-old woman. The gum line is necrotic and the interdental papillae are severely destroyed.
The connection between oral dysbiosis and the onset or worsening of systemic diseases is largely attributed to the persistence of a low-grade inflammatory state throughout the body, which is exacerbated by active inflammation in the oral cavity. The impact of the oral microbiome on systemic health can extend beyond local effects [6]. Some researchers suggest that oral bacteria or their metabolic byproducts may enter the bloodstream and migrate to other organs, potentially leading to complications in distant sites [39]. Many systemic diseases can be, closely or remotely, linked to oral dysbiosis, highlighting the oral microbiome’s impact on general health. Pathologies such as rheumatoid arthritis [40], chronic obstructive pulmonary disease (COPD) [41], obstetric complications [42, 43], Alzheimer’s disease [44], inflammatory bowel diseases [45], and cardiovascular disorders are associated with imbalances in oral microbiome (Fig. 6). In the remainder of this manuscript, we propose a more specific focus on infective endocarditis, diabetes, nutritional deficiencies, Alzheimer’s disease, chronic pulmonary disease, pregnancy outcomes and paediatrics.
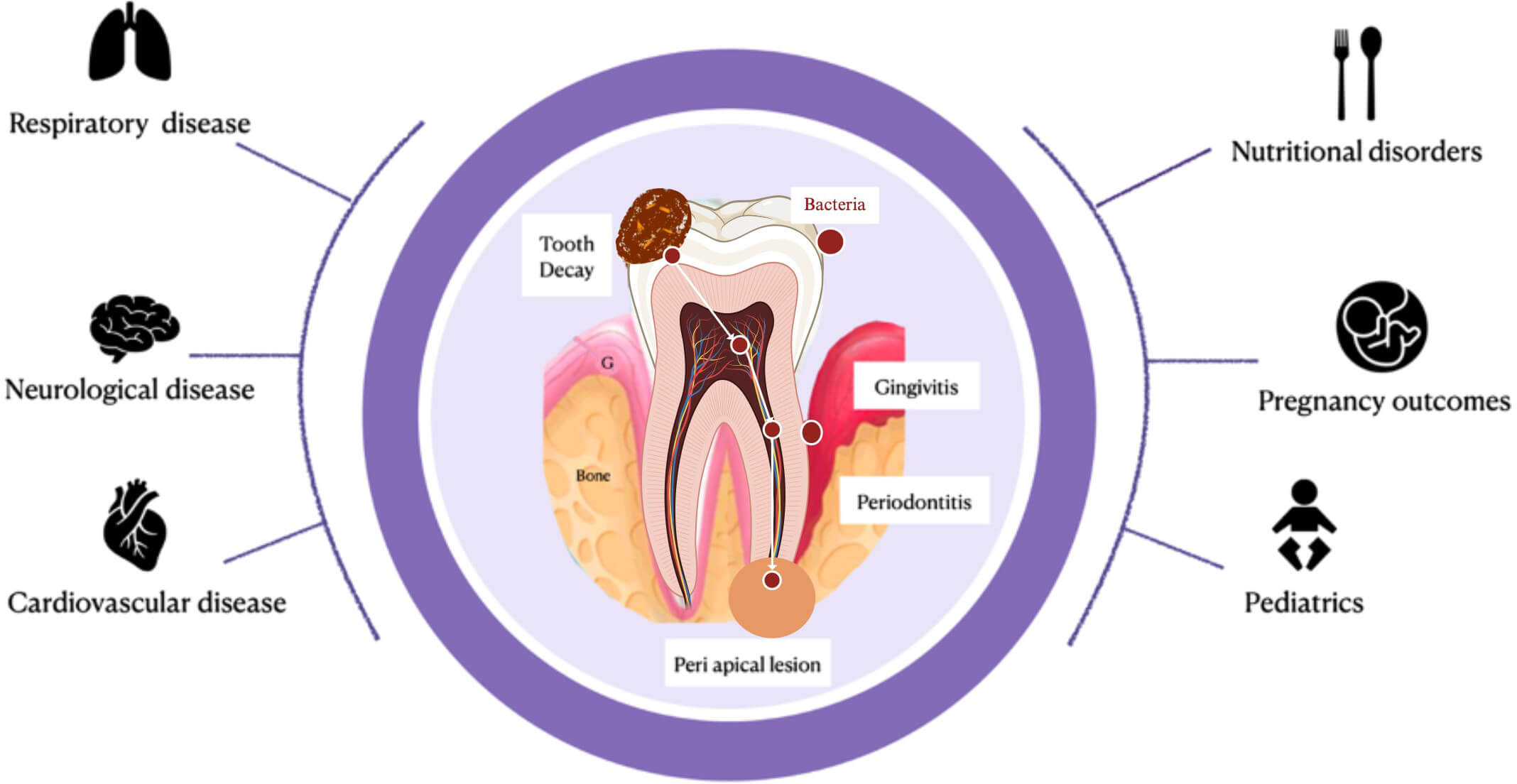 Fig. 6.
Fig. 6.
Schematic links between oral and systemic health. Figure designed with BioRender® (BioRender Inc., Toronto, Ontario, Canada; https://www.biorender.com/) and PowerPoint® (version 16.85, Microsoft Corporation, Redmond, WA, USA).
Infective endocarditis (IE) is a serious and often life-threatening infection of the heart’s inner lining, valves, or implanted cardiac devices, caused by bacteria entering the bloodstream and adhering to damaged heart tissues. Poor oral health is a significant risk factor for IE, as the oral cavity can serve as a reservoir for bacteria such as S.m., Streptococcus mitis (S.mi.), and other viridans group streptococci, which are involved in up to 50% of IE cases in the United States annually [46]. Once in the bloodstream, these bacteria can colonise heart valves or damaged endocardial surfaces, leading to infection [47]. People with predisposing conditions such as prosthetic heart valves, congenital heart defects or a history of IE are at particularly high risk [48]. While invasive dental procedures like tooth extractions have traditionally been associated with bacteremia and IE risk, experts explain that even the more basic daily procedures in the context of poor oral hygiene may represent an important threat [49]. The accumulation of plaque and calculus promotes periodontal disease, which not only exacerbates local inflammation but also increases systemic risks by facilitating bacterial dissemination [50]. Preventive measures such as maintaining good oral hygiene are essential to reduce bacterial load and prevent gingival bleeding. For high-risk patients undergoing invasive dental procedures, guidelines from organizations like the American Heart Association recommend antibiotic prophylaxis to minimise bacteremia risk [51]. However, there is growing consensus that improving overall oral health is a more effective strategy for reducing IE incidence than relying solely on prophylactic antibiotics. This underscores the need for integrated care between dental and medical professionals to safeguard cardiovascular health.
Diabetes, both type I and type II, significantly impact oral health, creating a
bidirectional relationship that affects both glycemic control and dental
well-being [52]. Moreover, periodontal diseases are recognised
as the sixth complication of diabetes [53]. This reciprocal
relationship suggests that treatment of any type of periodontal disease should
improve glycemic control in diabetic patients. However, studies differ on this
point. Conventional periodontal therapy, as it is available to the majority of
patients, seems insufficient [54], whereas intensive
therapy has positive effects on blood glycemia [55], thus
creating limitations in equality of access to relevant treatments for the
population [56]. What is proven is that people with
diabetes are at a higher risk of developing various oral health issues due to
elevated blood glucose levels [57]. High blood sugar increases
glucose rates in saliva [58], providing a favourable
environment for harmful bacteria to thrive and form plaque, leading to tooth
decay and gum disease. Diabetes can also reduce saliva production, causing dry
mouth (xerostomia), which further exacerbates dental problems by reducing the
mouth’s natural protective mechanisms [59].
Periodontal disease, the most common oral health complication in diabetes,
affects more than 60% of individuals with type I and type II diabetes [60]. Ultimately, the relationship between diabetes and oral
health is reciprocal [61]. Chronic periodontal
inflammation promotes systemic dissemination of pro-inflammatory mediators such
as Interleukin-6 (IL-6) and Tumor Necrosis Factor-alpha (TNF-
Nutritional deficiencies in vitamins B, C and D can affect periodontal tissues, increasing the risk of periodontitis, tooth mobility, and tooth loss. Vitamin insufficiency is common among elderly individuals, those with eating disorders, or in the context of various systemic diseases such as gastrointestinal diseases, liver diseases, kidney diseases, cancers, heart failure and endocrine disorders [65]. As of 1983, Dummett [66] described that deficiencies in vitamins B1, B2, B3, B5, B6, and B8 could manifest as erosions, vesicles, and sometimes glossitis, accompanied by hypersensitivity of the mucous membranes. They can also cause skin and mucosal lesions, such as dermatitis, angular cheilitis, stomatitis, and gingival ulcers, as well as a pellagra syndrome, which can worsen oral symptoms like glossitis, stomatitis and gingivitis [67]. A deficiency in vitamin B12 can cause a burning sensation on the tongue, known as glossodynia [68]. These nutritional deficiencies reduce the regenerative capacity of mucous membranes and promote opportunistic infections, such as candidiasis [69]. Low levels of vitamins B9 and B12 are also associated with a higher prevalence of periodontitis [70, 71], that’s why supplementation with vitamin B9 may reduce gingival inflammation and improve the condition of periodontal pockets [72]. Numerous studies have also shown that low serum levels of vitamin C are linked to a higher prevalence of periodontitis and greater disease severity, potentially leading to the destruction of the tissues supporting the teeth and tooth loss due to bone resorption [73, 74, 75, 76]. Vitamin C deficiency is famous in history as it can lead to scurvy [77], one of the most widespread diseases on ships during the last centuries [78]. Regarding vitamin D, low serum levels are also associated with a higher risk of periodontitis [79] as it can lead to a decrease in bone mineral density, which increases the risk of alveolar bone loss and weakens the dental bone support, thus increasing the risk of periodontitis [80]. Thus, vitamin D supplementation can reduce gingival inflammation, probably due to its anti-inflammatory properties [81].
Alzheimer’s disease (AD) is a neurodegenerative disorder characterised by
progressive memory loss, cognitive impairments, and executive dysfunction
[82]. Two main pathological mechanisms can explain AD: the
accumulation of amyloid plaques around neurons and neurofibrillary degeneration
associated with tau protein [83]. Inflammation,
particularly neuroinflammation, plays a crucial role in the progression of the
disease [84]. So, it is not surprising that recent
research has suggested that extrinsic factors, such as oral health issues, may
contribute to the progression of AD [85]. A specific link
has been established between periodontitis and AD [86].
Epidemiological studies have shown that individuals with periodontal problems,
such as tooth loss or the presence of deep periodontal pockets, are more likely
to develop cognitive impairments [87]. In a cohort study,
Kamer et al. [44] revealed that significant tooth loss in elderly subjects
was associated with faster cognitive decline. Furthermore, a link between
periodontitis and the Apolipoprotein E epsilon 4
(APOE-
First, pathogenic oral bacteria such as Porphyromonas
gingivalis (P.g.) produce toxins (gingipains) that can induce systemic
inflammation and, in particular, neuroinflammation
[89]. Recent studies suggest a potential link between
periodontal pathogens like Fusobacterium nucleatum (F.n.) and
Alzheimer’s disease [90], because this bacterium and its
virulence factors, like lipopolysaccharides (LPS), could cross the blood-brain
barrier, particularly in older individuals or those genetically predisposed to AD
[91]. In animal models, the introduction
of P.g. promoted the accumulation of amyloid-
The upper respiratory tract is an extension of the oral cavity, making the mouth a potential reservoir for respiratory pathogens. Chronic Obstructive Pulmonary Disease (COPD) is an inflammatory lung condition characterised by symptoms such as difficult breathing, chronic cough, excessive mucus production, and wheezing [96]. Although bronchodilators and anti-inflammatory drugs are first-line treatments for COPD, they are not always effective in controlling infectious exacerbations. In fact, the use of inhaled corticosteroids in patients with COPD and chronic bronchial infections can even increase bacterial load in the airways and raise the risk of pneumonia. In this context, long-term or intermittent antibiotic treatment has been shown to prevent COPD exacerbations and hospitalisations [97, 98]. Recent research has highlighted a connection between periodontitis and COPD [99]. Bacteria from periodontal tissues can easily contaminate the airways through the oral cavity, further worsening COPD symptoms. A study showed that bacterial diversity was higher in patients with COPD, with the Lachnospiraceae family often present in both periodontitis and COPD patients [100]. Conversely, treatments for COPD, particularly inhaled medications, can negatively affect oral health. These treatments are associated with dental issues such as periodontitis, dry mouth, oral mucosal ulcers, gingivitis, and taste alterations [101]. Inhaled corticosteroids also increase the risk of Candida infections [102] (Fig. 7). Co-infections involving bacteria like F.n. and Pseudomonas aeruginosa (P.a.) may also play a crucial role in respiratory inflammation [103]. Therefore, managing oral health in COPD patients is essential not only for preventing dental infections but also for reducing exacerbations of lung disease.
 Fig. 7.
Fig. 7.
Candidiasis of the inner mucosa of the cheeks in a woman, due to inhaled corticosteroids treatment (Becotide®, GSK, France).
Oral health significantly impacts pregnancy outcomes and maternal well-being. Poor oral health during pregnancy has been linked to several adverse effects, including preterm delivery, low birth weight babies, and pre-eclampsia [104]. Several studies have demonstrated the possible translocation of oral bacteria into the placenta, which may play a role in complications during pregnancy [105, 106]. The hormonal changes during pregnancy, particularly increased levels of estrogen and progesterone, make women more susceptible to gum problems like gingivitis (Fig. 8) and periodontitis [107]. A study shows that pregnant women are more prone to oral diseases: they are 1.97 times more likely to develop dental caries [107] and nearly 47% suffer from periodontitis [42].
 Fig. 8.
Fig. 8.
Gravidic gingivitis in a patient 6 months pregnant, manifested by hypertrophy and bleeding of the gums.
Certain medications used for oral health issues can also potentially affect the developing fetus if taken during pregnancy. Tetracycline antibiotics should be avoided as they can cause discolouration of the child’s developing teeth [108]. Nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated, and benzodiazepines used for dental anxiety should be avoided due to potential risks to the fetus [109].
Recognising the importance of oral health during pregnancy, healthcare professionals recommend regular dental check-ups, proper oral hygiene habits, and preventive care to ensure the well-being of both mother and child [110]. Despite the reluctance of dentists, dental care can be performed during pregnancy, and has positive effects on both the future mother and the unborn child. In France, for example, a national program called “M’T Dents” (a wordplay that could be translated as “Love your teeth” in English), funded by the social security system, provides a free dental check-up for every pregnant woman. Timely treatment of oral health issues, while keeping in consideration the safety of medications, can help prevent complications and ensure better pregnancy outcomes.
The development of human dentition begins early in life, even before birth, then continues during childhood with the emergence of primary teeth. While primary teeth share anatomical features with their permanent counterparts, they possess distinct characteristics. They are smaller, lack tight contact points, and have a more globular appearance with a milky hue [111]. Surprisingly, some babies can be born with small, often highly mobile, natal teeth (Fig. 9), which can be extracted in the first few hours of life to avoid any risk of inhalation [112]. Maternity unit medical teams should be systematically prepared for this eventuality.
 Fig. 9.
Fig. 9.
Neonatal teeth of a 7-day-old child requiring extractions.
Children’s dental care requires particular attention, as primary teeth are surprisingly vulnerable to rapid decay processes. Infections in these early teeth are not merely isolated incidents but can have profound implications for future permanent dentition, such as enamel defect, shape alteration and delayed or ectopic eruption [113]. Modern preventive strategies emphasise a holistic perspective. Regular dental hygiene involves more than traditional brushing; it encompasses understanding dietary impacts, recognising early warning signs, and implementing proactive maintenance protocols. Fluoride-based products, balanced nutrition, and limiting sugar consumption emerge as fundamental protective measures. Parental education plays a crucial role in this preventive paradigm to transform passive care into an active, informed approach to maintaining children’s oral well-being.
Emerging researches continue to underscore the importance of early, comprehensive dental care, positioning prevention as the most effective strategy in managing oral health challenges [114, 115]. The impact of oral health on children’s overall well-being extends far beyond the confines of the oral cavity. Poor oral health in children can have significant systemic consequences, affecting various aspects of their physical and psychological development. Untreated dental caries and periodontal diseases can lead to chronic pain, difficulties in eating and speaking, and sleep disturbances, all of which can impair a child’s growth, cognitive development, and academic performance [116]. Moreover, oral infections can potentially spread to other parts of the body, leading to more serious conditions such as endocarditis or brain abscesses in rare cases [117]. Chronic oral inflammation has been associated with systemic diseases later in life, including cardiovascular diseases and diabetes. Psychosocially, visible dental problems can negatively impact a child’s self-esteem and social interactions [118], potentially leading to behavioural issues and reduced quality of life [119, 120]. Additionally, early childhood caries has been linked to increased risk of developing caries in permanent teeth, underscoring the long-term implications of maintaining good oral health from an early age [121]. These interconnections between oral and systemic health emphasise the critical importance of early prevention, regular dental check-ups, and proper oral hygiene habits for the promotion of overall health and well-being in children.
Hospital dentistry plays a central role in ensuring comprehensive and coordinated healthcare by bridging the gap between oral health and systemic well-being [122]. Its integration within hospital settings is essential for delivering patient-centred care, particularly for individuals with complex medical conditions. By fostering interdisciplinary collaboration, hospital dentistry enhances the quality and safety of care across multiple medical specialities [123]. For instance, in oncology, pre-treatment dental screenings are critical for identifying and eliminating potential oral infection sources, thus preventing serious complications during chemotherapy or radiotherapy [124]. Similarly, in cardiology and cardiac surgery, the involvement of dental professionals in pre-operative assessments helps prevent oral-origin infections that could compromise surgical outcomes [125]. Hospital dentistry also contributes significantly to emergency care by providing specialised management of oral infections and trauma, ensuring timely and effective interventions.
A distinctive strength of hospital dentistry lies in its ability to provide treatment under general anesthesia for patients with special needs, such as those with severe intellectual or physical disabilities, extreme dental phobia, or complex comorbidities that preclude conventional dental treatment [126]. General anesthesia enables the delivery of comprehensive dental care in a single session, reducing patient stress and ensuring optimal treatment conditions. This approach is particularly beneficial for young children who are unable to cooperate due to age, anxiety, or developmental challenges [127].
Although general anesthesia involves inherent risks, its benefits often outweigh the potential complications, when accompanied by appropriate pre-operative evaluation, intra-operative monitoring, and post-operative care protocols [128]. Ultimately, by ensuring access to essential oral healthcare for vulnerable and medically complex populations, hospital dentistry not only promotes health equity but also underscores the importance of multidisciplinary collaboration in modern healthcare systems.
Recent research has clearly established that oral health is deeply interconnected with systemic health. Central to this relationship is the role of the oral microbiome and its influence on inflammation throughout the body. Oral dysbiosis can trigger local and systemic inflammatory responses, contributing to the development or aggravation of diseases such as diabetes and cardiovascular disorders.
This emerging understanding is reshaping medical practice: dental assessments are increasingly recognised as essential components of the prevention and management of systemic diseases. Integrating oral healthcare into multidisciplinary care pathways enhances treatment efficacy and reflects a more holistic vision of patient well-being.
As scientific evidence continues to grow, strengthening the systemic implications of oral health, interdisciplinary collaboration between dental and medical professionals will be crucial for advancing prevention, diagnosis, and patient care.
All data, figures and literature references included in this study are available from the corresponding author upon reasonable request.
MMi, VBB and TC designed the sections of this review. AP, LD, and CT performed the literature check and contributed to data acquisition. SL, MMa and LD designed the figures on Biorender software and contributed to the analysis. AP, LD and MMa drafted the manuscript. TC managed the whole work. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The consent of all patients concerned by the publication of photographs or X-rays was obtained on paper. In the case of the child, consent was obtained from both parents. This study was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki.
Not applicable.
This research received no external funding.
Fig. 1 and Fig. 6 were created using BioRender (https://www.biorender.com/). The authors have no financial or personal relationship with BioRender, and the use of this tool does not imply any endorsement. The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.