
Introduction: The incidence of malignancy in pregnancy is reported to range approximately between 0.02% and 1%. Synovial sarcoma (SS) is a rare aggressive mesenchymal tumor for which there are no treatment guidelines during pregnancy. Case Report: The authors report a 23-year-old primigravida presenting, at 20+0 weeks of pregnancy, with a growing painful mass in the left thigh. The diagnosis of monophasic SS grade 3 was confirmed by the presence of SYT gene fusion. On MRI scan there was a heterogeneous localized mass of size 75×115×103 mm, but there was no evidence of distant metastases. Limb-sparing surgery with clear-surgical margins was performed at 26+3 weeks of pregnancy. Adjuvant chemotherapy with two cycles of doxorubicin was followed by delivery of normal child by caesarean section at 36+3 weeks of pregnancy. Adjuvant radiotherapy of total dose of 66 Gray to the site of the resection had been administered followed by two cycles of doxorubicin. Conclusion: The patient is free of recurrence six months after the completion of the treatment.
Pregnancy-associated malignancy is defined as a neoplastic disease diagnosed during pregnancy or within one year after delivery [1]. The incidence of cancer during pregnancy reported in the literature ranges between 0.02% and 1% [2-5]. Due to the low incidence rate and to the fact that the clinical symptoms may be attributed to or disguised by changes during the pregnancy, cancer in pregnant women is often diagnosed late [1]. Limited experience with malignant disorders associated with pregnancy further increases diagnostic confusion [6, 7]. The last 20 years have seen a growing trend in the incidence of pregnancy-associated cancer in the Western world as reproduction plans are made at a later age [8]. The most frequently diagnosed malignancies during pregnancy are breast carcinoma, cervical carcinoma, ovarian carcinoma, thyroid carcinoma, melanomas, lymphomas, leukaemia and colorectal carcinoma [1, 2, 7, 9, 10]. Bone and soft tissue sarcomas are a very heterogeneous group of malignant tumors. Malignant bone tumours represent 0.2%, most commonly osteosarcoma, Ewing’s sarcoma, and chondrosarcoma [10]. The incidence of soft tissue sarcomas is about 1% [11]. A number of soft tissue sarcomas have been reported during pregnancy, including liposarcoma, rhabdomyosarcoma, fibrosarcoma, synovial sarcoma (SS), neurosarcoma, hemangiopericytoma, leiomyosarcoma, myxoma, and unclassified sarcomas [7]. SS comprise 8-10% of all soft tissue tumours that are very rarely encountered during pregnancy [10, 12]. Due to the limited data in the literature, it is also unclear how these tumours behave during pregnancy [13-15]. In this report the authors present an extremely rare case of monophasic SS of the lower extremity diagnosed at 20+0 weeks of gestation and review the literature.
A 23-year-old primigravida/nullipara at 20+0 weeks of gestation was referred from an orthopaedic department of a regional hospital, where an aspiration of presumed haematoma located ventromedially in the proximal part of the left thigh was performed. Cytology showed suspicious cells. The patient had noticed a swelling of the thigh for the last six weeks that became larger and painful during the last three weeks. The family history included breast cancer of her mother at 30 years of age, the mother’s mother was treated for a breast cancer, and the father’s mother treated for stomach cancer. Personal history was insignificant. Peripheral blood cell count and serum biochemistry were also unremarkable. MRI scans showed a non-homogeneous bounded layer with a central necrosis in the groin area and adductors to the left approximately 75×115×103 mm in total size (Figures 1 and 2). The staging examinations including a whole-body MRI scan demonstrating no evidence of distant metastases (Figure 3). Immunohistochemistry showed expression of vimentin, calponin, CD 99, BCL-2, CD 34, CD 31m and CD 56, while AE 1/3, CK18, EMA, H-caldesmon, SMA, sarcomeric actin, HHF-35, S100, myogenin, CD 10, HMB-45, melan A, chromogranin, and synaptophysin were negative. The histological finding of spindle cells and immunohistochemical markers indicated the diagnosis of monophasic SS, grade 2. The detection of the translocation of the SYT gene using the fluorescence in situ hybridization (FISH) method confirmed the diagnosis. The multi-disciplinary team decided on a primary surgical treatment in an orthopaedic department specialised in oncology surgery. At 26+3 weeks of gestation, tumour resection was performed in collaboration with a vascular surgeon. The excised encapsulated tumour measured a total of 110×80×60 mm. No sign of infiltration of the capsule was observed. Minimal clear margin of 1 mm was obtained. The histological examination confirmed the diagnosis of SS, but in contrast with the initial biopsy, the definitive tumour grading was G3 (Figure 4). At 31+1 weeks of gestation the first cycle of adjuvant chemotherapy with doxorubicin (60 mg/m2) was administered. The second cycle followed three weeks later. At 36+3 weeks of gestation, a cesarean section was indicated. A baby girl weighing 2,540 grams was born. Due to respiratory distress syndrome, the child was admitted for distension therapy in the intensive care unit, but was discharged on the ninth day after birth in a good clinical condition. The mother ceased to lactate. An ultrasound examination of the scar showed no presence of residual tumour. A post-natal full-body MRI scan showed a suspicious nodule in the left groin (Figure 5). Adjuvant radiotherapy to the total dose of 66 Gray in 33 fractions to the site of the tumour had been administered followed by two cycles of doxorubicine (60 mg/m2) with every three weeks check up. Resection of the node had been performed and histological examination showed no SS. At the last follow up visit in March 2018, the patient is six months without any evidence of disease recurrence.
 Figure 1.
Figure 1.— MRI scan of the left thigh showing a non-homogenous well-demarcated mass with central necrosis (size 75×115× 103 mm, transversal view).
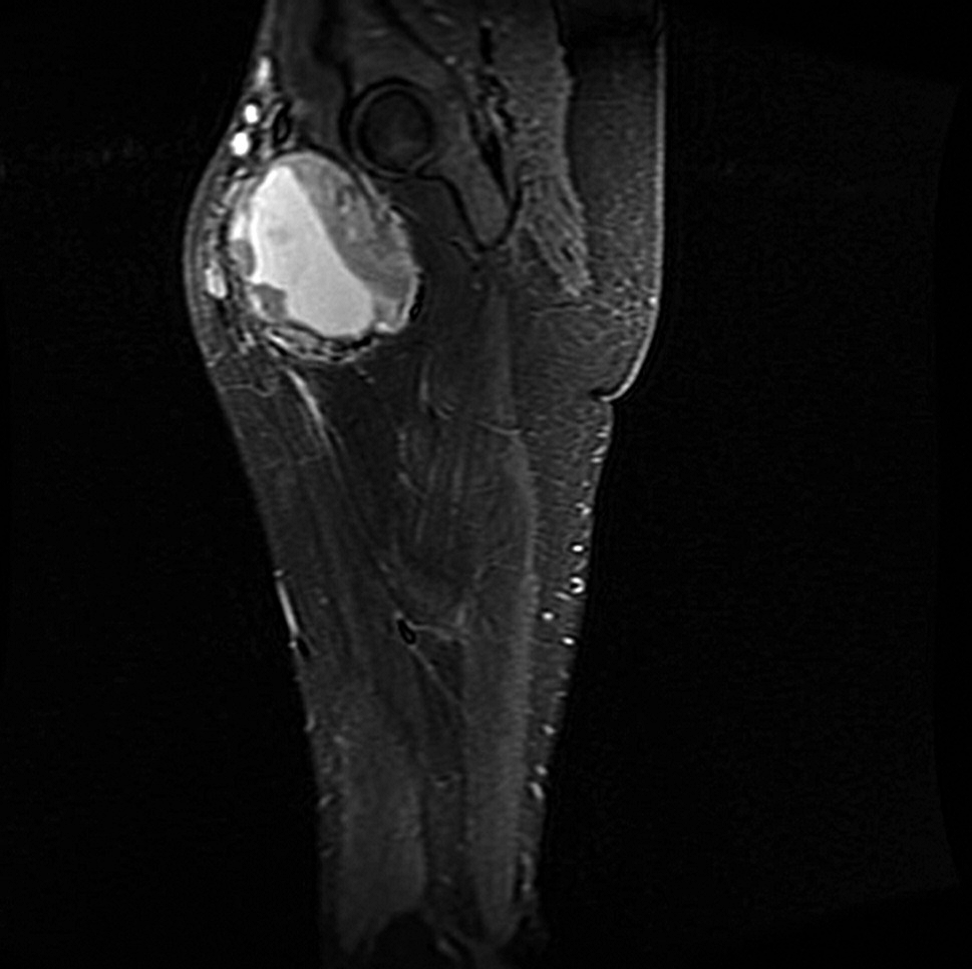 Figure 2.
Figure 2.— MRI scan of the left thigh showing a non-homogenous mass with central necrosis (size 75×115×103 mm, sagittal view).
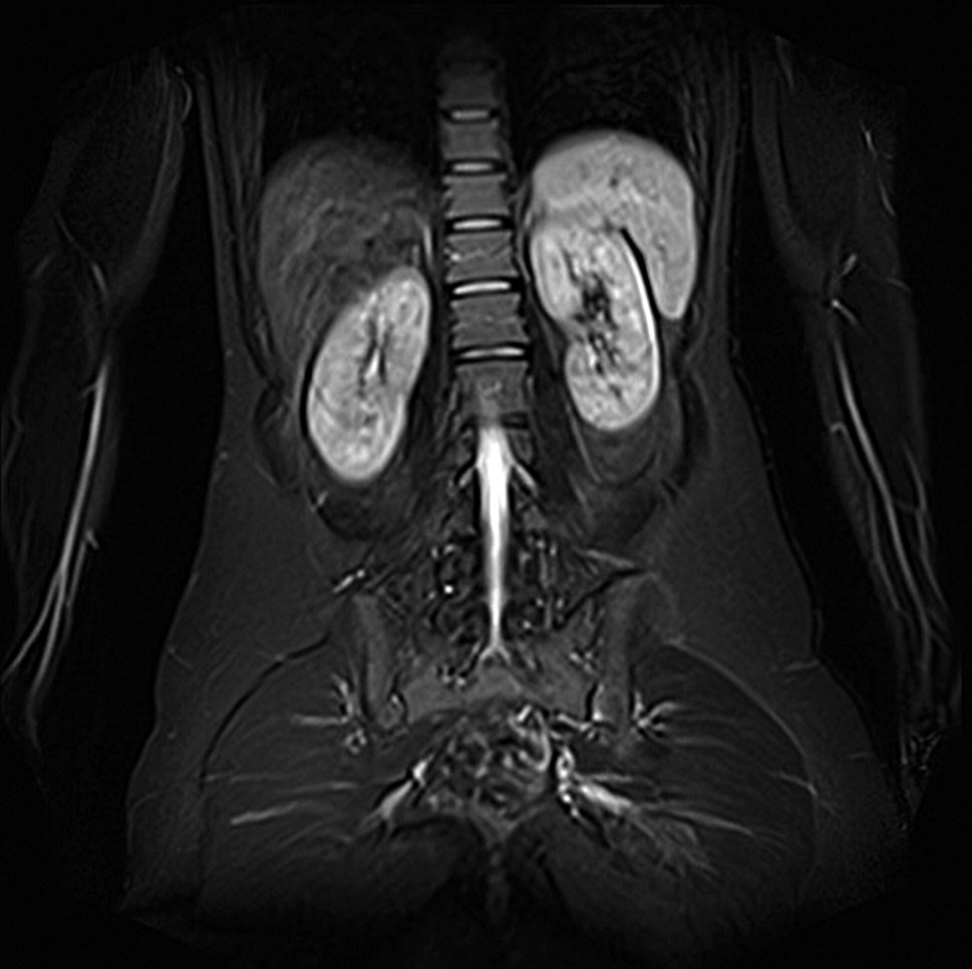 Figure 3.
Figure 3.— Full body MRI scan with no signs of distant metastasis (coronal view).
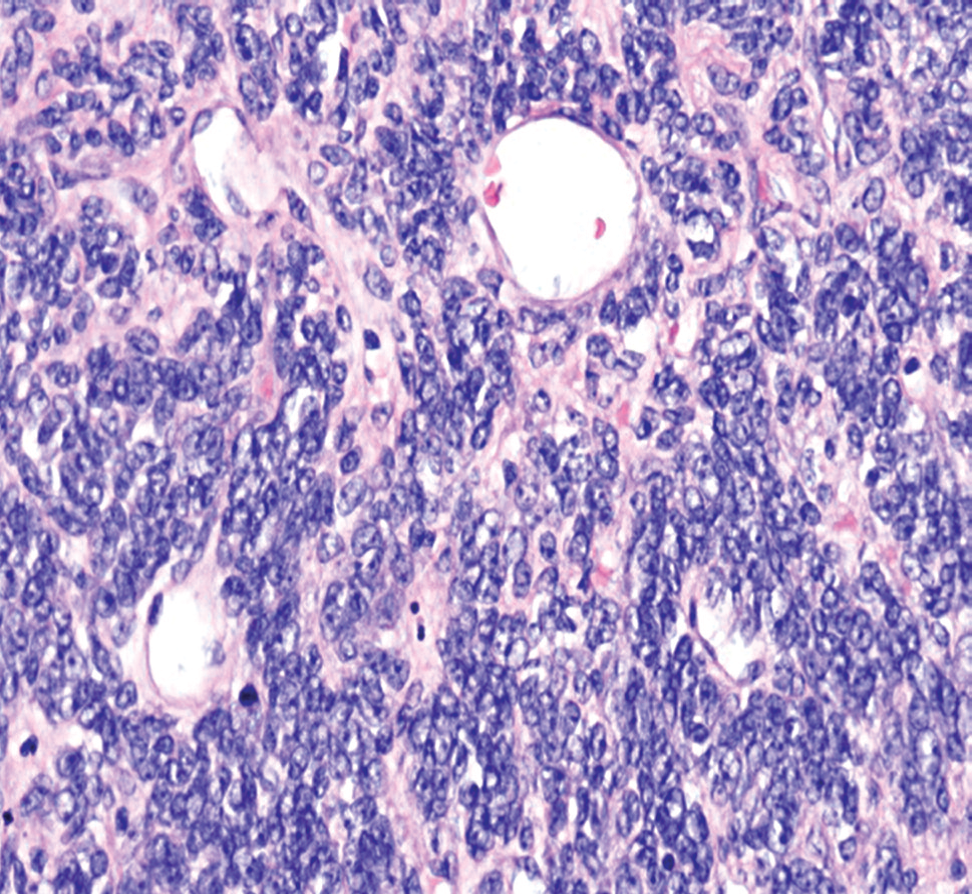 Figure 4.
Figure 4.— H&E staining ×400. Synovial sarcoma; G3. Irregular oval-shaped cells can be seen. Extracellular matrix is slightly less collagenous. The nuclei are rounded-oval shaped, hyperchromatic, but uniform.
 Figure 5.
Figure 5.— MRI scan of the left thigh. The image shows enlarged lymphatic node with malignant features (coronal view).
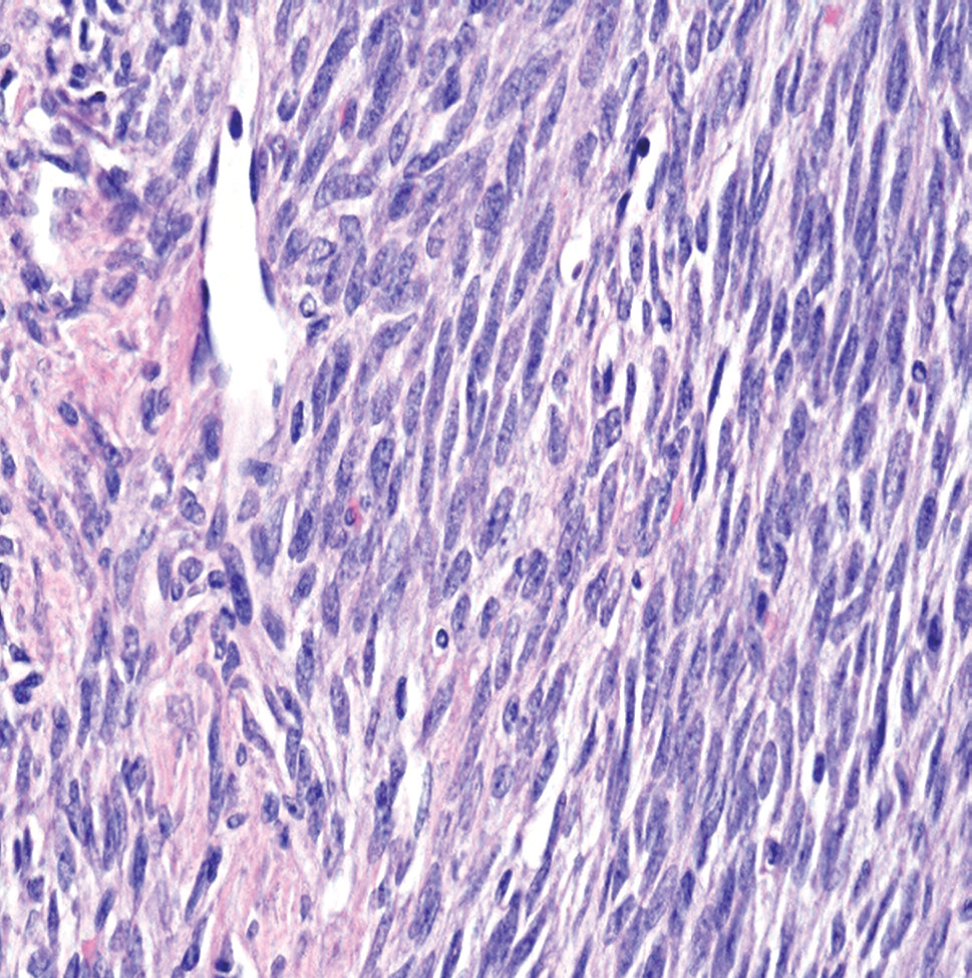 Figure 6.
Figure 6.— H&E staining ×400.Synovial sarcoma; G2. Ovalshaped cells growing in irregular fascicles can be seem. Extracellular matrix is slightly less collagenous. The nuclei are oval shaped, and at one end slightly tapered.
The authors present here an extremely rare case of SS diagnosed during pregnancy. Up to 2017, only a total of nineteen cases of pregnancy-associated SS had been reported in the literature worldwide. Of these 19 published cases, two involved recurrences [16, 17]. The remaining seventeen case reports described primary manifestation of the disease during pregnancy. All cases of SS are reviewed in Tables 1, 2, and 3. SS is a mesenchymal tumour of unclear histological origin [18]. Despite the name, SS does not grow solely from synovial cells. SS is generally localised in the vicinity of the joints, tendons, and synovial bursae, most often on the lower extremity, specifically in the area of the knee and the ankle [19]. The tumour is most frequently multi-nodular with infiltration of the soft tissues and, occasionally, propagation into the neurovascular bundles. SS has also been described outside synovial tissue, including the esophagus, retroperitoneum, chest wall, pleura, heart, pericardium, lungs, prostate, abdominal wall, sacrum, iliopsoas muscle, pharynx, tonsils, 3rd cerebral ventricle, and vulva. SS has also been reported in the orofacial, intraosseous, and intravascular regions [20]. The possibility of SS should always be considered in the differential diagnosis when finding a tumour with spindle-shaped cells in an unusual location. The most frequently described primary site of SS in pregnancy (six cases in the literature) is the lower extremity, as in the present case. Another frequent primary location is the lung (five cases reported in the literature). In two cases, the tumour originated from the kidney and has also been described in the adrenal gland, retroperitoneum, orofacial region, hypopharynx, pleural cavity, anterior abdominal wall, and omentum. SS typically presents as a gradually expanding painful mass that grows slowly and insidiously [19, 21]. This presentation was typical in nine cases reported in the literature. Other presenting signs and symptoms were associated with the tumour site, including urinary and respiratory problems [19, 21]. One patient presented with deep vein thrombosis and another was hospitalised with suspected pre-eclampsia. In general, it may be stated that SS could occur at any age [22, 23]. However, the prevalence is the highest in the group between the age of 15 and 40 years [19, 21]. Literature comprises a total of 19 patients aged from 19 to 38 years, with a mean age of 30 years. Diagnostic imaging uses all routinely available methods including X-ray, ultrasound, CT, and MRI scan. The last mentioned method has demonstrated the highest accuracy in soft tissue tumours [23]. SS does not have any characteristic presentation with any of these imaging techniques. If possible, a biopsy is always performed in order to determine the diagnosis. Three histological SS subtypes have been described including monophasic, biphasic, and poorly differentiated SS [24]. The monophasic type contains a spindle-shaped cell component. Biphasic SS contains, alongside spindle shaped cells, and epithelial cells arranged into glandular structures [24]. Immunohistochemically, SS typically expresses vimentin, cytokeratin, epithelial membrane antigen, as well as S100 and CD 34, the latter two are usually poorly reactive [25]. In the present case, the SS expressed vimentin, calponin, CD 99, BCL-2, CD 34, CD 31, and CD 56. A balanced reciprocal translocation of the 18th chromosome with subsequent fusion of the SYT gene is pathognomonic of SS [24]. This translocation is detected in more than 90% of SS cases [26]. Reverse transcriptase-polymerase chain reaction (RT-PCR) or FISH are used for diagnosis [27]. A correlation exists between the type of fusion transcript and the histological SS subtype. The SYT-SSX1 translocation is typical of biphasic sarcomas, while the SYT-SSX2 translocation is most often detected in monophasic sarcoma. The type depends on sarcoma morphology. Hemmings and Fisher also described the presence of the SYT-SSX4 gene [20]. In the present case, fusion of the SYT-gene was demonstrated using FISH and led to the definitive diagnosis. The presence of the SYT-SSX gene in the peripheral blood of pregnant woman suffering from SS was determined using RT-PCR in two cases [20, 28]. Hemmings and Fisher believe, similarly to Hashimoto et al., that measuring the level of these genes in the peripheral blood could be used to monitor the effect of chemotherapy or to detect disease relapse. SS was diagnosed in all trimesters of pregnancy [20, 28]. One pregnancy reported in the literature was terminated in the first trimester because of this diagnosis [29]. In the case presented by Vernooy et al., there was rapid progression of the disease leading to maternal death in the 24th week of pregnancy [17]. Premature births were recorded in nine cases. Eight babies were delivered by cesarean section and three vaginally. In six patients, data relating to the type, timing, and other details concerning the termination of pregnancy are lacking. The patient in the present report also delivered her baby prematurely by a cesarean section at week 36+3 because of planned adjuvant therapy. The recommended optimal treatment of localised forms of SS includes primary surgery followed by adjuvant treatment. Preoperative chemotherapy or radiotherapy may be effective in the case of primary inoperable tumours. As in other soft-tissue sarcomas, the role of adjuvant chemotherapy is not completely clear. In patients with pregnancy-associated sarcoma, radiotherapy appears to be most suitable following delivery [10, 19]. SS are sensitive to doxorubicin and ifosfamide [27]. It is preferable to defer administration of chemotherapy until after the end of the first trimester due to the risk of toxicity to the fetus. In the subsequent weeks of pregnancy, the developing eyes, central nervous system and haematopoetic tissue are most sensitive to chemotherapy. Administration of chemotherapy in the second and third trimesters may lead to growth retardation [22]. In the case reports of patients reported in the literature, doxorubicin, cisplatin, and ifosfamide were administered during pregnancy. Radiotherapy was usually not planned until after delivery. However, in two cases, radiotherapy was administered during pregnancy. Orlandi et al. described the use of radiotherapy after thorough shielding in the area of the head and neck from the 23rd week of pregnancy until delivery in the 36th week [4]. Tachibana et al. administered radiotherapy from the 22nd to the 26th week of pregnancy in the case of a recurrence of primary SS of the shoulder in the lungs [16]. A healthy newborn was observed in both these cases. In the published cases, therapy was indicated individually depending on disease extent and maximum efforts were made to reduce adverse effects on the fetus. Given the location of the disease in the present case, the patient was indicated to undergo limb-sparing surgery during the second trimester. This was followed in the third trimester by adjuvant chemotherapy involving two cycles of doxorubicin. After delivery, the patient received adjuvant radiotherapy and chemotherapy, which was interrupted because of suspected local recurrence, and the patient underwent surgery. Limb-saving surgery was described in two published cases; however, data on the extent of the surgical procedure were not available in the case of other patients [7, 19]. Adverse prognostic factors in SS include tumour size over 5 cm, male gender, age at diagnosis over 20 years, advanced tumour necrosis, high grade, number of mitoses over ten, neurovascular invasion, and the SYT-SSX1 variant. The most adverse prognostic factor is incomplete resection of the tumour [26]. Enzinger and Weiss cite a 70-83 % recurrence rate in the case of incomplete resection. In the case of complete resection and subsequent adjuvant radiotherapy, recurrence decreases to 28-36% [11]. Dvorak et al. cite a five-year overall survival ranging from 27-76%; followed by a ten-year survival of 20-63% [23]. SS metastasizes into the lungs, lymph nodes, and bone marrow [21, 23]. According to Adamesteanu et al. recurrence and/or metastatic disease occurs in up to 80% of cases [19]. In the case of SS tumours described in pregnancy, patient death was reported in seven cases. Death may be presumed in at least one additional case, given the advanced stage of the disease, an early recurrence and patient refusal to undergo systemic treatment (Table 3). However, the follow up was very short in most of the remaining cases reported.
| Case number | Reference | Age | Primary site | Histology and grade | Time of diagnosis in relation to pregnancy | Clinical presentation |
|---|---|---|---|---|---|---|
| 1 | Merimsky, O., Cesne, A., L. [7] | 26 | Knee | Synovial sarcoma; G3 | 3 months after delivery | Enlargement of a pre-existing cyst |
| 2 | Merimsky, O., Cesne, A., L. [7] | 31 | Cuboid bone | Synovial sarcoma; G3 | 2nd trimester | Painful mass at the site of resection of necrotic bone |
| 3 | Acton, C., M., Morrison, W.,A., Slavin, J., L. [21] | 20 | Popliteal fossa | Synovial sarcoma; G2 | Postpartum | Soft tissue mass |
| 4 | Hashimoto, N. et al. [28] | 22 | Thigh | Synovial sarcoma; G3 | 24th week of pregnancy | Enlarging painful mass |
| 5 | Dvorak, M. et al. [23] | 30 | Thigh | Biphasic synovial sarcoma | 3rd trimester | Deep vein thrombosis |
| 6 | Adamesteanu, M., O. et al. [19] | 19 | Thigh | Biphasic synovial sarcoma; G3 | 15th week of pregnancy | Enlarging painful mass |
| 7 | Harris, E., M., Allan, R., W., Riggs Jr., Ch. E. [12] | 26 | Lungs | Monophasic synovial sarcoma | 21th week of pregnancy | Dry cough, pleuritic chest pain |
| 8 | Esaka, E., J., et al. [26] | NR | Lungs | Synovial sarcoma; G3 | 34th week of pregnancy | Shortness of breath, dyspnea, chest pain, pneumothorax |
| 9 | Bunch, K., Deering, S., H. [27] | 38 | Lungs | Synovial sarcoma; G3 | 26th week of pregnancy | Dyspnea, orthopnea, upper right back pain |
| 10 | Tachibana, D. et al. [16] | 30 | Lungs /recurrent SS/ | Synovial sarcoma | 15th week of pregnancy | Not specified /treated for SS of arm at 24 years of age/ |
| 11 | Sakurai, H. et al. [25] | 33 | Pleural cavity | Synovial sarcoma | ND | Spontaneous haemothorax |
| 12 | Nebhnani, D. et al. [29] | 25 | Kidney | Monophasic synovial sarcoma | 8th week pregnancy | Enlarging painful mass in the flank, haematuria |
| 13 | Bettendorf, O. et al. [13] | 32 | Kidney | Monophasic synovial sarcoma | 32th week of pregnancy | Painful haematuria |
| 14 | Gonin, J. et al. [14] | 28 | Adrenal gland | Synovial sarcoma G3; sarcomatoid carcinoma; Ewing tumour | 26th week of pregnancy | Abdominal pain, suspected preeclampsia |
| 15 | Orlandi, E. et al. [4] | 23 | Cheek | Biphasic synovial sarcoma | 22th week of pregnancy | Enlarging painful mass |
| 16 | Ortiz, M., Giraldez, L., A., Riera-March, A. [9] | 23 | Hypopharynx | Synovial sarcoma | 2nd trimester | Acute airway obstruction |
| 17 | Kanade, U., S. et al. [6] | 21 | Anterior abdominal wall | Biphasic synovial sarcoma | 34th week of pregnancy | Enlarging painful mass |
| 18 | Hemmings, Ch., Fischer C. [20] | 37 | Omentum | Synovial sarcoma | 1st trimester | Lower abdominal pain |
| 19 | Vernooy, C., B. et al. [17] | 28 | Retroperitoneum /recurrent SS/ | Synovial sarcoma | 14th week of pregnancy | Painful mass of the left flank /treated for SS of the same location in 13 years of age/ |
ND: no data;
| Case number | Reference | Diagnostic methods used during pregnancy | Timing of treatment | Diagnostic algorithm and treatment during pregnancy |
|---|---|---|---|---|
| 1 | Merimsky, O., Cesne, A., L. [7] | Physical examination | After delivery | Biopsy, neoadjuvant chemotherapy |
| 2 | Merimsky, O., Cesne, A., L. [7] | Physical examination, X-ray | 3rd trimester | Limb sparing surgery |
| 3 | Acton, C., M., Morrison, W.,A., Slavin, J., L. [21] | Ultrasound | After delivery | Excision+ wide reexcision |
| 4 | Hashimoto, N. et al. [28] | MRI scan | 27th week of pregnancy | Limb sparing surgery and observation |
| 5 | Dvorak, M. et al. [23] | Ultrasound, MRI scan, CT scan, scintigraphy, DSA | After delivery | Neoadjuvant chemotherapy |
| 6 | Adamesteanu, M., O. et al. [19] | No exminations in pregnancy | 1 month after delivery | Not treated in pregnancy |
| 7 | Harris, E., M., Allan, R., W., Riggs Jr., Ch. E. [12] | CT scan, bronchoscopy, biopsy | 2nd trimester | Neoadjuvant chemotherapy |
| 8 | Esaka, E., J., et al. [26] | X-ray, CT scan, video-assisted thoracoscopy | 3rd trimester | Induction of labour |
| 9 | Bunch, K., Deering, S., H. [27] | X-ray, CT scan, CT guided biopsy | 2nd trimester | Pneumectomy+lymphadenectomy |
| 10 | Tachibana, D. et al. [16] | CT scan | 22th-26th.week of pregnancy | Neoadjuvant radiotherapy |
| 11 | Sakurai, H. et al. [25] | ND | ND | ND |
| 12 | Nebhnani, D. et al. [29] | CT, MRI scan | After MTP | NA |
| 13 | Bettendorf, O. et al. [13] | Ultrasound, MRI scan | 34th week of pregnancy | NA |
| 14 | Gonin, J. et al. [14] | Ultrasound, MRI scan | 27th week of pregnancy | NA |
| 15 | Orlandi, E. et al. [4] | MRI scan, biopsy | 23th week of pregnancy | Resection of the lesion, adjuvant radiotherapy from 30th-36th week of pregnancy |
| 16 | Ortiz, M., Giraldez, L., A., Riera-March, A. [9] | NR | Postpartum | Emergency tracheotomy and tumor debulking |
| 17 | Kanade, U., S. et al. [6] | MRI scan, biopsy | NR | Total excision of the mass |
| 18 | Hemmings, Ch., Fischer C. [20] | Ultrasound, minilaparotomy with excision of suspected omental pregnancy | 24th week of pregnancy | Debulking of the mass |
| 19 | Vernooy, C., B. et al. [17] | MRI scan, X-ray |
Not treated | Not treated |
NA: not applicable; ND: no data; NR: not reported;
| Case number | Reference | Timing and the method of delivery, newborn outcome | Treatment after delivery | Subsequent outcome |
|---|---|---|---|---|
| 1 | Merimsky, O., Cesne, A., L. [7] | Healthy baby | Planned for operation, adjuvant radiotherapy | NR |
| 2 | Merimsky, O., Cesne, A., L. [7] | Vaginal delivery, healthy baby | Local recurrence after 1 month, adjuvant chemotherapy, amputation followed by chemotherapy | NR |
| 3 | Acton, C., M., Morrison, W.,A., Slavin, J., L. [21] | Vaginal delivery | Adjuvant radiotherapy | NR |
| 4 | Hashimoto, N. et al. [28] | Vaginal delivery in 38th week of pregnancy, healthy baby | Adjuvant chemotherapy | DFS 18+ months |
| 5 | Dvorak, M. et al. [23] | Vaginal delivery | Neoadjuvant chemotherapy | Died 6 months after delivery |
| 6 | Adamesteanu, M., O. et al. [19] | C-section at term | Limb sparing surgery, adjuvant chemotherapy and radiotherapy | Follow up without relapse |
| 7 | Harris, E., M., Allan, R., W., Riggs Jr., Ch. E. [12] | C-section in 31th week of pregnancy due to foetal distress, premature healthy baby | Neoadjuvant chemotherapy, surgery - total pneumectomy + mediastinal lymphadenectomy | Recurrence after 5 months, died 13 months after diagnosis |
| 8 | Esaka, E., J., et al. [26] | Preterm induction of labour, vaginal delivery, healthy baby | Pneumectomy, adjuvant chemotherapy | Died 13 months after surgery |
| 9 | Bunch, K., Deering, S., H. [27] | C-section in 32th week of pregnancy due to FGR, baby required surgical closure of pulmonary artery | Adjuvant radiotherapy due to metastatic disease 4 weeks after delivery | Died 6 weeks after delivery |
| 10 | Tachibana, D. et al. [16] | C-section in 30th weeks of pregnancy due metastatic disease, at 30 months of age normal development | NR | Died 33 months after delivery |
| 11 | Sakurai, H. et al. [25] | ND | ND | ND |
| 12 | Nebhnani, D. et al. [29] | MTP | Radical nephrectomy, adjuvant chemotherapy | DFS 6+ months |
| 13 | Bettendorf, O. et al. [13] | C-section in 34th week of pregnancy, healthy baby | Adjuvant chemotherapy and radiotherapy followed by chemotherapy | DFS 8+ months |
| 14 | Gonin, J. et al. [14] | C-section in 27th week of pregnancy due foetal distress, satisfying condition of the baby | C-section+ adrenalectomy, lymphadenectomy, adjuvant chemotherapy and radiotherapy | DFS 8+ months |
| 15 | Orlandi, E. et al. [4] | C-section in 36th week of pregnancy, healthy baby, at 8 months normal development | Adjuvant radiotherapy | DFS 8+ months |
| 16 | Ortiz, M., Giraldez, L., A., Riera-March, A. [9] | Spontaneous preterm labour in 29th week of pregnancy | Partial pharyngectomy | DFS 30+ months |
| 17 | Kanade, U., S. et al. [6] | NR | Adjuvant radiotherapy and chemotherapy - refused treatment | 6 months after delivery multiple metastatic disease, lost to follow up |
| 18 | Hemmings, Ch., Fischer C. [20] | C-section in 32th week of pregnancy + preoperative multiple sites biopsy | Adjuvant chemotherapy | 9 month after delivery recurrent tumour, debulking surgery, 2 line chemotherapy, died 36 months after diagnosis |
| 19 | Vernooy, C., B. et al. [17] | NA | NA | Died in 24th week of pregnancy |
DFS: disease-free survival; DSA: digital subtraction angiography; FGR: foetal growth retardation; G: grade; MTP: medical termination of pregnancy; NA: not applicable; ND: no data; NR: not reported; SS: synovial sarcoma.
The incidence of malignancy in pregnancy is 0.02-1%. Given the generally increasing trend in the incidence of cancer, it is highly probable that the incidence in pregnancy will also rise. SS is very rare in pregnancy and only case reports are available in literature. There are no recommended guidelines for the treatment, which must always be individual, based on the location of the primary lesion, malignant potential, and disease spread. In fact, case reports and small case series like the present review are the only data available to support decisions on how to manage the patients with this extremely rare condition. Treatment of pregnant women is modified, as the goal is to minimise adverse effects on the fetus. It should be always planned by a multidisciplinary team.