
Aim: Our study aims to characterize the differential efficacy of
martensitic and austenitic files in root canal retreatment regarding defiling
ability, debris management and morphometric features. Materials and
methods: A total of 10 human premolar teeth with two separate fully formed roots
were selected, prepared with BioRace system (BR) up to a size BR2 (0.04/25). Root
canals were filled and then divided according to the file type into two groups (n
= 10). Two geometrically identical files have been used with the only difference
between them is heat treatment; One Curve (OC) martensitic and One Shape (OS)
austenitic. Preoperative and postoperative Micro-CT scans were done for all the
samples, and the percent volume of residual filling materials was calculated.
Canals reshaping and remaining debris in the canals were assessed by calculating
the volume of the canals before and after retreatment using Micro-CT software.
Results: The percentages of removed filling materials were similar
between both groups (97.2% OC vs 97.8% OS). OS was significantly faster than OC
(P
NiTi endodontic rotary files have been used for the cleaning and shaping during endodontic treatment to eliminate infection from inside the root canal. The enhanced flexibility and super elasticity of these files allow them to negotiate sever canal curvatures without separation and with minimal alteration to the original anatomy of the root canal. Two main phases of these NiTi files are associated with the shape memory and super elasticity, martensite and austenite, with R-phase as intermediate phase that may occur [1]. The effect of these phases on the mechanical properties of NiTi files have been studied in the literature. A previous report showed that there is a correlation between stress point localization during file bending and cross section geometry, therefore it is recommended to move the file in and out during rotation inside the canal to distribute internal stresses along the file length [2]. Also, it was shown that the presence of R-phase because of heat treatment improved file flexibility [3]. Different geometrical factors can also affect the file behavior and characteristics. A finite element analysis study showed that the polar moment of inertia is the most important factor in determining file’s torsional resistance over cross sectional area and metal mass [4].
Complete removal of endodontic materials is crucial for the success of nonsurgical root canal retreatment as it enables efficient cleaning, disinfection, shaping, and filling of the root canal system [5]. Conservative access design is also recommended to save coronal tooth structure while allowing efficient instrumentation of the root canal system [6].
The removal of filling materials from the root canal system has been implemented using multiple techniques, including the use of endodontic Gates Glidden burs, hand files, heat, ultrasonic instruments, nickel-titanium (NiTi) rotary files, laser, and use of adjunctive solvents [7, 8]. Nonetheless, none of the previous studies have shown the ability to completely remove root canal filling materials [9], especially in the apical portion of root canals [10]. Remaining filling materials inside the root canal prevents the complete disinfection of the root canal and also prevents the bonding of root canal sealer into dentin walls. However, the use of NiTi rotary files in root canal retreatment is proved to be more effective than hand instruments with fewer procedural errors [11, 12]. Thus, different rotary systems have been developed by several manufactures to optimize gutta-percha removal techniques.
ProTaper Universal Retreatment system (Dentsply Maillefer, Ballaigues, Switzerland) has been used as an alternative to hand files for removing gutta-percha in endodontic retreatment cases [12]. The system has three files, D1, D2, and D3, where each one is used for each root canal third, according to the manufacturer [13, 14].
Different reports showed that when ProTaper retreatment files are used, they leave between 10 and 35% of gutta percha remnants behind. Therefore, it is recommended to use supplementary files [14, 15].
The removal of gutta-percha with ProTaper retreatment files with or without the use of self-adjusting file was evaluated, it was found that the gutta-percha was not completely removed from the apical portion of curved canals. However, using SAF enables the removal of more gutta-percha than ProTaper alone [15].
Reciprocating single-file systems, originally designed for root canal instrumentation, were suggested to be used for root canal retreatment [16, 17, 18]. Their reciprocating motion increases the instrument’s resistance to cyclic fatigue [19, 20], and when compared to rotational and hand files, they were shown to be more efficient in the removal of gutta percha from the root canal walls [19].
The use of 2 reciprocating systems, i.e., WaveOne and Reciproc was compared with a continuous rotation system (ProTaper Universal Retreatment). Both Wave One and Reciproc reciprocating systems were as efficient as the ProTaper Universal retreatment system in removing sealer and gutta-percha [9].
Although different nickel-titanium (NiTi) files were developed [21],extensive research has been done to modify the presently available root canal instrument designs, modifying the surface of the alloy or changing the alloy microstructure with post-twisting or post machining heat treatment [22].
Single file systems use was introduced and recommended to use to reduce cross-contamination and instrument fatigue. Thus, minimizing instrument separation within the canal without compromising the cutting efficiency [23].
One Shape single file system (OS) is based on one instrument composed of electropolished austenite 55-NiTi alloy. The OS single instrument is used in a full clockwise rotation with a constant taper of 0.06 with variable cross-sections across the length of its active working part and a tip size of 25 mm [24]. This innovative asymmetrical cross-section with a longer pitch increases the available volume for upward debris elimination allowing better shaping. More flexibility is also gained because of the longer instrument pitch, which provides an increased ability to navigate curves and allows easy instrument progression to the apex [24, 25].
One Curve single file system (OC) is a heat-treated OS NiTi file, made of martensite C-Wire, which is an exclusive proprietary, developed by the manufacturer. It is claimed to be hyperflexible with increased cyclic fatigue resistance without sucking effect. The tip size comes in multiple sizes, i.e., 25, 35, and 45 with either 4% or 6% taper [26].
Both systems OS and OC, have a similar design with a unique asymmetrical cutting profile and an inactive tip to maintain the original canal curvature and therefore may cause less transportation [27].
From a clinical point of view, added to the inability to completely remove root canal filling materials, root canal retreatment procedures can result in transportation of root canals that could lead to ledging, perforation, zipping, especially in the apical third [28]. Thus, these conditions should be examined, which can lead to the prevention of root weakening and to reduce the possibility of vertical root fracture or canal perforation. To date, there are few studies about the efficacy of filling material removal in natural canals using single-file NiTi systems. Furthermore, the ability of OS and OC systems in removing filling material from natural canals has not been evaluated yet. Therefore, the present study aimed to compare One Shape and One Curve single file systems regarding filling material removal efficiency, the working time needed for filling removal, and canal morpho geometry changes after retreatment through certain parameters such as canal volume, surface area, SMI, straightening, transportation, un- instrumented canal surface area, and debris removal.
Ten double-rooted teeth with canal curvature (10–20
Teeth were divided randomly into two groups with 10 canals per group (n = 10) according to the rotary file used for retreatment. In group A (n = 10), OC was used and in group B (n = 10), OS was used. Both systems were used at 600 rpm with 2.5 N/cm to improve their retreatment efficiency and penetration capability. Complete removal of the filling materials was verified by a dental operating microscope (Zeiss, Munich, Germany) and periapical radiographs.
All teeth were inserted in special micro-CT holders to ensure accurate
positioning between scans. The samples were scanned with a commercially available
cabinet micro-CT (
Data was checked and we excluded the outliers prior to any statistical analysis
performed. Normality of pre retreatment data distribution was tested suing the
Shapiro-Wilk test, which showed normally distributed data [29]. Mean and standard
deviation was calculated for all parameters. Statistical analysis was performed
using IMB® SPSS® (PASW version 23.0
IBM®, Chicago, IL, USA). The paired sample t-test was
used for statistical analysis between pre and post retreatment data for each
group. The unpaired sample t-test was used for statistical analysis
between post retreatment data in the two groups. The P-value for
statistical significance was set at
There was no statistically significant difference in the volume of filling
materials before retreatment between both groups (P
| Variable | One Curve n = 10 | One Shape n = 10 | P-value |
| Initial filling material (mm |
1.90 |
1.67 |
0.437 |
| Filling material removed (%) | 97.38 |
97.87 |
0.595 |
| Time in seconds | 308.80 |
262.20 |
0.001 |
| Volume (mm |
0.46 |
0.40 |
0.724 |
| Area (mm |
1.62 |
1.42 |
0.721 |
| SMI | 0.28 |
0.27 |
0.927 |
The morpho geometric changes created by OC and OS files in the root canals were
analyzed. The results did not show statistically significant differences between
both groups in terms of pre-retreatment measurements (P
Three dimensional rendered images were constructed showing concatenated root canals of the pre-and post-retreatment scans, Fig. 1. The green color shows the pre-retreatment root canal geometry, and the orange shows post-retreatment root canal geometry. Cross-section slices were taken from raw micro-CT data at level slices 701, 901, and 1201 of both pre-and post-retreatment scans, Fig. 2.
 Fig. 1.
Fig. 1.Three dimensional rendered images of concatenated root canals of the pre- and post-retreatment scans. Green color shows the pre-retreatment root canal geometry and orange shows post-retreatment root canal geometry. (A) shows palatal view of the root canals. (B) shows mesial view of the root canals. (C) shows buccal view of the root canals. (D) shows distal view of the root canals.
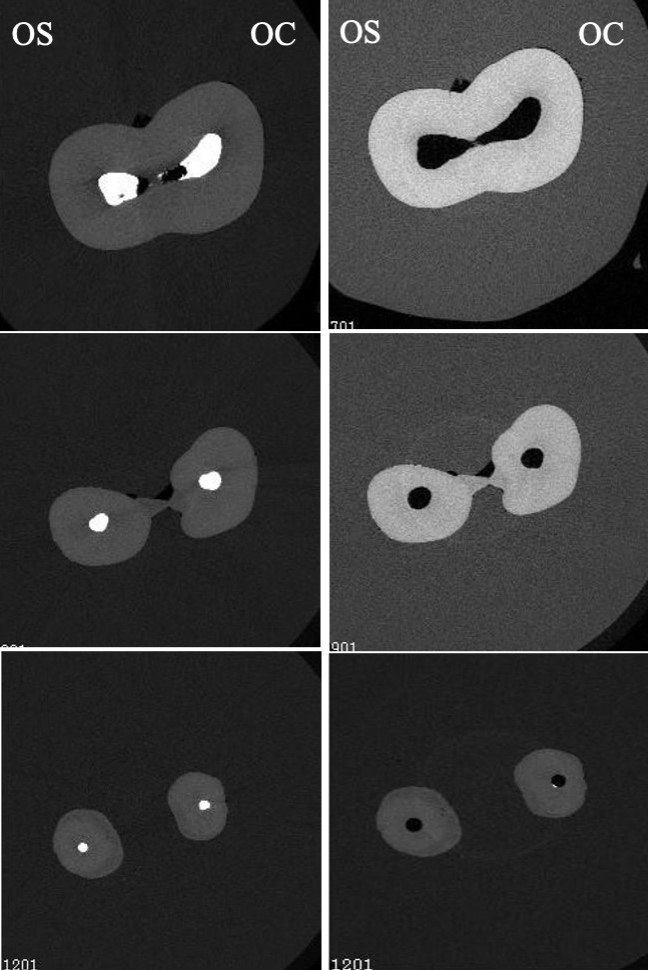 Fig. 2.
Fig. 2.Cross section slices taken from raw micro-CT data at level slices 701 (top) 901 (middle), and 1201 (bottom) of both pre- and post- retreatment scans. Cross sections on the left side show pre- retreatment images and cross sections on the left show images of post-retreatment.
Canal straightening for OC and OS groups was 13.93% (
| Variable | One Curve n = 10 | One Shape n = 10 | P-value | |
| Mean canal transportation | Coronal third | 29.2600 |
33.5400 |
0.656 |
| Middle third | 31.8000 |
35.7400 |
0.792 | |
| Apical third | 33.5600 |
86.2600 |
0.047 | |
| Un-instrumented Static voxels | 23500.20 |
21027.90 |
0.605 | |
| Un-instrumented canal surface area (%) | 40.32 |
41.28 |
0.915 | |
| Percentage reduction of debris | 96.97 |
95.82 |
0.263 | |
The mean volume of accumulated hard tissue debris (AHTD) before and after
retreatment was calculated. There are no statistically significant differences in
the experimental groups before or after retreatment (P
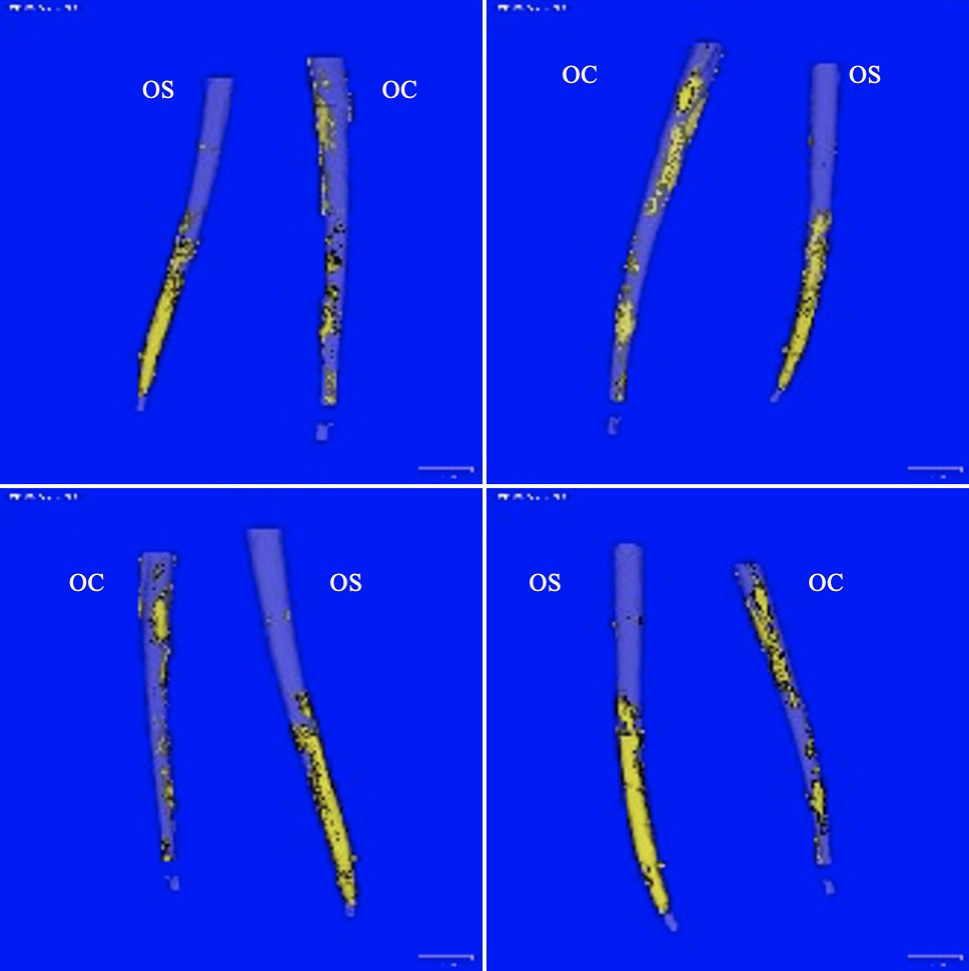 Fig. 3.
Fig. 3.Different views of three-dimensional computer constructed images of root canal system showing the amount of hard tissue debris after retreatment with either OC (One Curve) or OS (One Shape) files.
Recent advances in the metallurgical engineering of NiTi instruments led to the development of various NiTi rotary files that are manufactured by different heat treatment such as max-wire, c-wire, t-wire, controlled memory (CM), R-phase, and M-wire [30, 31, 32, 33]. Different heat-treated files exhibit different phase transformation behavior, which improves fatigue resistance, torsional reissuance, and flexibility [34, 35, 36, 37, 38]. Heat-treated NiTi rotary files are available in two forms, martensitic and austenitic with wide range of motion kinematics, cross section, design, and sizes, which may result in biased shaping ability results.
In the study, we aimed to compare the differential efficacy of two heat-treated rotary files systems which are only different in their metallurgical properties, austenite (OS) and martensite (OC), in the ability to remove gutta-percha from root canals, the time needed for removal, and the morpho geometric changes created during the removal.
The main objective of root canal retreatment is the disinfection of the root canal system which leads to healing of the periapical tissues. Studies have reported that the successful outcome of root canal retreatment ranges from 87 to 97% depending on whether preoperative periapical periodontitis was present or absent [39]. One of the factors that affect the outcome in cases of endodontic retreatment is the ability to completely remove the previous filling material from the root canal [40, 41].
Micro-computed tomography (
Micro CT analysis was used in our study to evaluate the removal of failing materials as well as to evaluate the morphometric changes created in the root canals after the use of two different rotary systems, One Curve, and One Shape. None of the previous retreatment studies show that it is possible to remove 100% of the filling materials from the root canals [5, 40, 44, 45, 46]. However, in this study, both systems were able to remove around 97% of filling material compared to 75–81% in a previous study in which ProTaper rotary files were used with solvent for retreatment [5]. The mean time to remove gutta-percha ranges from 262 seconds by OS to 308 seconds by OC compared to 540–720 seconds in a study by Mittal 2014 and 412–532 seconds in a study by Giuliani, 2008 [5, 47]. These results come in agreement with previous studies in which the use of rotary instruments resulted in shorter working times [7, 46, 48, 49]. However, other reports show opposing results in which root canal retreatment was achieved using hand instruments compared to rotary instruments [40, 50].
In other parts of this study, the morpho geometric changes in the root canals were observed. The shaping ability of rotary files can be affected by several factors, such as instrument design (cross-section, taper, size, and the number of flutes), motion kinematics (reciprocation, adaptive rotation, continuous rotation, or oscillation), and the number of instruments used [43, 51, 52, 53]. In this study, all these variables were standardized except for file metallurgy between OC (martensitic) and OS (austenitic). Martensitic files such as OC are characterized by enhanced flexibility and controlled memory. However, OS files with its austenitic crystal arrangement tend to be harder and stiffer [32]. This difference in flexibility could be the reason why OS files were able to remove gutta-percha from the root canals in a statistically significant shorter time than OC files. Pretreatment parameters such as volume, area, and SMI did not show significant differences. However, OC shows a statistically significant increase in SMI which was not shown in a study in which canals were not filled with gutta-percha [53]. This means that OC files resulted in more round canals then OS files, which can be explained by the increased flexibility of OC files [32]. When it comes to canal straightening and apical transportation, OS showed a significant increase compared to OC, which comes in agreement with a previous report [53]. This can also be explained by the decreased flexibility of OS file and absence of controlled memory feature [32]. We can assume that the thermomechanical treatment of the files exerted its effect on the behavior of the files inside the root canal especially when it comes to canal straightening and apical transportation. On the other hand, in a study by Almeida et al. [54], there was no statistically significant difference between the heat-treated K3FX files and the superplastic conventional K3 in terms of canal transportation using the same methodology for quantification. However, superior results were found in terms of canal transportation with the use of ProTaper Gold compared to conventional ProTaper Universal [55].
Both OS and OC files showed a significant reduction in accumulated hard tissue debris with no statistically significant difference between both files. This indicates that both files can be used during root canal retreatment for gutta-percha removal.
Limitations of the study are the use of only one type of sealer and only one technique of obturation. Future studies could focus on the retreatment ability to remove bioceramic sealers from root canal walls.
Both OS and OC files were unable to completely remove gutta-percha 100% from the root canal with a significantly shorter time using OS for retreatment. OS showed a significant increase in canal straightening and apical transportation, while OC files touched more canals walls. According to our results, both files can be used for root canal retreatment, however OC files should be used in curved and narrow canals and OS should be used in more straight and wide canals.
LA—Draft preparation, writing, review, and editing. WR—Formal analysis, methodology, and investigation. MA-H—Writing, review, and editing. HA—Data curation. YA—Resources. KB—Project administration and validation.
The study is in accordance with the guidelines of the Ethical Review Committee, Faculty of Dentistry, King Abdulaziz University, Jeddah 21589, Saudi Arabia.
Thanks to all the peer reviewers for their opinions and suggestions.
This research was funded by The Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, Saudi Arabia, grant number G-1347-165-1440.
The authors declare no conflict of interest.