
 , Esme Ekizoğlu 2, Halime Arıkan 3, Bahar Taşdelen 4, Aynur Özge 5, Paolo Martelletti 6
, Esme Ekizoğlu 2, Halime Arıkan 3, Bahar Taşdelen 4, Aynur Özge 5, Paolo Martelletti 61 Spine Health Unit, Faculty of Physical Therapy and Rehabilitation, Institute of Health Sciences, Hacettepe University, 06100 Ankara, Turkey
2 Department of Neurology, Istanbul Faculty of Medicine, Istanbul University, 34093 Istanbul, Turkey
3 Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Tokat Gaziosmanpasa University, 60000 Tokat, Turkey
4 Department of Biostatistics and Medical Informatics, Mersin University School of Medicine, Mersin University, 33343 Mersin, Turkey
5 Department of Neurology, Algology and Clinical Neurophysiology, Mersin University School of Medicine, 33343 Mersin, Turkey
6 Department of Clinical and Molecular Medicine, Sapienza University, 00185 Rome, Italy
Abstract
Background: Pharmacological treatment is the primary approach in chronic migraine (CM), although non-drug interventions such as physical therapy are used as adjunct treatments. We aimed to review the efficacy of physical therapy and rehabilitation approaches for CM and their impact on quality of life (QoL) and disability. Methods: This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and included randomized controlled trials (RCTs) in adults with CM. The primary outcomes were changes in intensity, frequency, duration of headache, disability, and QoL. Methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) scale. Data synthesis and quantitative analysis were conducted on relevant studies. Results: Seven RCTs were included in the narrative review, and five of them were eligible for quantitative analysis. Aerobic exercise (AE), osteopathic manipulative treatment (OMT), occipital transcutaneous electrical stimulation (OTES), acupressure, hydrotherapy, instrument-assisted soft tissue mobilization (IASTM), facial proprioceptive neuromuscular facilitation (FPNF), and connective tissue massage (CTM) were used in CM. AE combined with pharmacological therapy reduced the frequency, duration, and intensity of headache. OMT combined with medication improved QoL and reduced disability, intensity of pain, and migraine days per month. Hydrotherapy combined with medication also resulted in improvements in the intensity of headache, frequency, and overall QoL. IASTM and OTES reduced the intensity of headache, alleviated neck pain, and improved QoL, although there were conflicting findings following OTES alone on disability and intensity of headache. Both FPNF and CTM reduced the intensity of headache. Acupressure as an adjunct to medication did not show additional benefits on the intensity of headache and QoL. Quantitative analysis of the data showed that manual physical therapy combined with medication reduced the intensity of headache (p = 0.0796), and manual or AE combined with medication reduced the headache days per month (p = 0.047). Conclusions: A limited number of RCTs investigating the efficacy of physical therapy and rehabilitation approaches show promise in improving headache symptoms, reducing disability, and enhancing QoL in CM. Meta-analysis of the data also supported favorable outcomes for both intensity and headache days per month. Further research is needed to better understand the efficacy, optimal duration, and safety of physical therapy and rehabilitation approaches for CM, and to explore alternative interventions.
Keywords
- chronic migraine
- physical therapy
- rehabilitation
- exercise
- manual therapy
- intensity of headache
- headache frequency
- disability
- quality of life
- randomized controlled trials
Migraine significantly impacts individuals’ lives and its management necessitates a multidisciplinary approach [1, 2, 3, 4, 5]. The global prevalence of migraine is estimated to be 15–18% [6], with chronic migraine affecting approximately 1–2% of the general population. Chronic migraine often develops from episodic migraine, with an annual progression rate of about 3%, resulting in an increased frequency of attacks [7, 8]. Various risk factors, including female sex, high initial attack frequency, stressful life events, low educational status, obesity, ineffective acute treatments, snoring, and overuse of acute migraine medications, contribute to the progression of migraine [9, 10]. Compared with episodic migraine, chronic migraine significantly impacts social, physical, and occupational functioning, leading to reduced health-related quality of life (HR-QoL) [11, 12, 13].
Pharmacological agents are the primary treatment approach for migraine [14, 15, 16, 17]. However, some patients may not benefit sufficiently from drug therapy or may experience side effects leading to discontinuation or inadequate dosing [18]. In such cases, non-drug interventions, including physical therapy, acupuncture, relaxation techniques, or exercises, are often used as adjunct treatments for the management of chronic migraine [19].
The main objective of this study was to review the efficacy of physical therapy and rehabilitation approaches for chronic migraine, as well as their impact on the quality of life (QoL) and disability associated with headache attacks in these patients. Furthermore, we aimed to assess the methodological quality of the studies conducted in this field.
This systematic review was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the protocol was registered in PROSPERO (the number: CRD42023392051, https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=392051). PRISMA checklist is shown in Supplementary Material.
The review question was formulated using the PICOS (Participants, Intervention, Comparison, Outcome, Study design) framework: “Do physical therapy and rehabilitation approaches improve the intensity of headache, frequency, duration, disability, and QoL in patients with chronic migraine?” (P: Patients with chronic migraine; I: Physical therapy and rehabilitation approaches; C: Comparison group (healthy or placebo); O: Intensity of headache, frequency, duration, disability, QoL; S: This systematic review and meta-analysis include randomized controlled studies that compare the effectiveness of physical therapy and rehabilitation approaches on intensity of headache, frequency, duration, disability, and QoL in chronic migraine).
A comprehensive literature search was conducted in the PubMed and Web of Science databases, covering the period from the inception of the databases to January 29, 2023. No language restrictions were applied. A meta-analysis was subsequently performed using the available quantitative data. The search strategy utilized specific keywords, which are listed in Appendix.
For inclusion in this systematic review and meta-analysis, we considered human randomized controlled trials (RCTs) conducted in adults aged 18 years and older who were diagnosed with chronic migraine, with or without aura. We excluded animal studies, studies involving children and adolescents below 18 years of age, abstracts, case reports or series, letters to the editor, retrospective-prospective cohort studies, case-control studies, review articles, conference proceedings, articles published in non-peer-reviewed journals, theses, dissertations, and studies focusing on headaches other than chronic migraine.
The process of study selection involved two steps. Initially, the articles retrieved from the literature search were screened based on their titles and abstracts, using the predefined inclusion and exclusion criteria. Subsequently, the full texts of the remaining articles were assessed to determine their eligibility for inclusion in the review. Two independent researchers conducted the searching and screening process, ensuring a thorough and unbiased selection of studies.
The methodological quality of the included RCTs was assessed using the Physiotherapy Evidence Database (PEDro) (https://pedro.org.au/) scale. The PEDro scale comprises 10 items, each with a binary response of YES (positive rating) or NO (negative rating). The total score on the scale determines the quality rating, with scores below 4 indicating poor quality, scores of 4–5 indicating fair quality, scores of 6–8 indicating good quality, and scores of 9–11 indicating excellent quality [20]. Two independent researchers (D.O and H.A) evaluated the methodological quality of the studies based on the PEDro scale.
Data extraction was performed to collect relevant information on trial and patient characteristics. This included details such as the country of recruitment, sample size in each arm, mean age of participants, and gender distribution. Additionally, information on the interventions used and outcome measures assessed in the studies were also collected. The primary outcomes of interest were defined as the alterations in intensity, frequency, and duration of headache attacks, as well as the impact on disability and QoL among individuals with chronic migraine. The data extraction process was conducted by the researchers to ensure accuracy and consistency in gathering the necessary information from the included studies.
The outcome measures used in the included trials were evaluated, and a
frequentist random-effects meta-analysis was conducted to analyze the
quantitative data of the common outcome measures. Before conducting
meta-analysis, the mean change in each group was obtained by subtracting the
post-intervention mean from the baseline mean. Standard deviations of the changes
were available for only one study [21] and we used these values as a reference
(SD
and similarly for the control group (Corr
The I
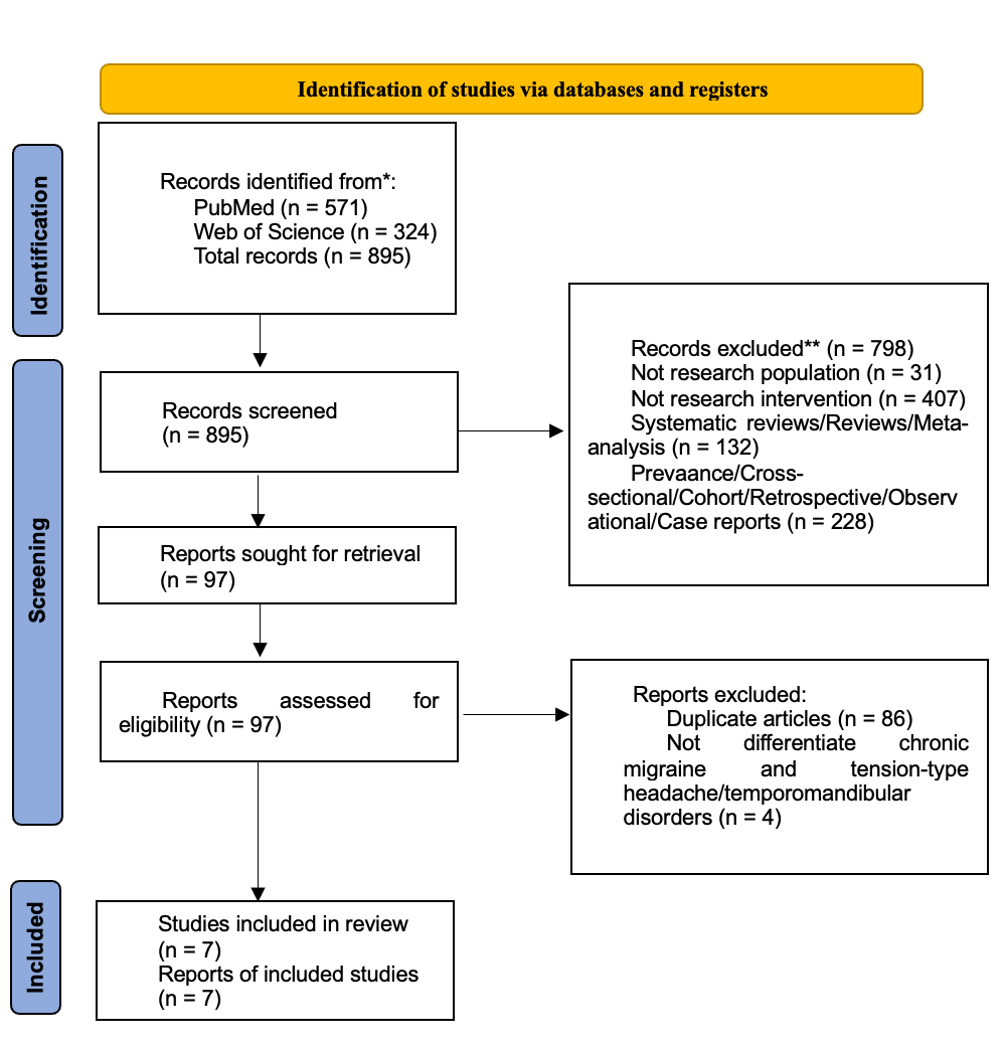
In this systematic review and meta-analysis, a total of 895 records were initially screened, and after applying our inclusion criteria, seven RCTs were deemed eligible for narrative review. All included studies were written in English. The study selection process is depicted in the PRISMA flowchart diagram (Fig. 1), providing a visual representation of the selection process. The selected studies varied in terms of study design, country of recruitment, sample size, mean age, gender distribution, interventions, treatment duration, and outcome measures. Out of the seven studies, five [21, 23, 24, 25, 26] shared common outcome measures such as intensity of headache [21, 23, 24] and the number of headache days per month [21, 25, 26], making them eligible for further quantitative analyses in our meta-analysis.
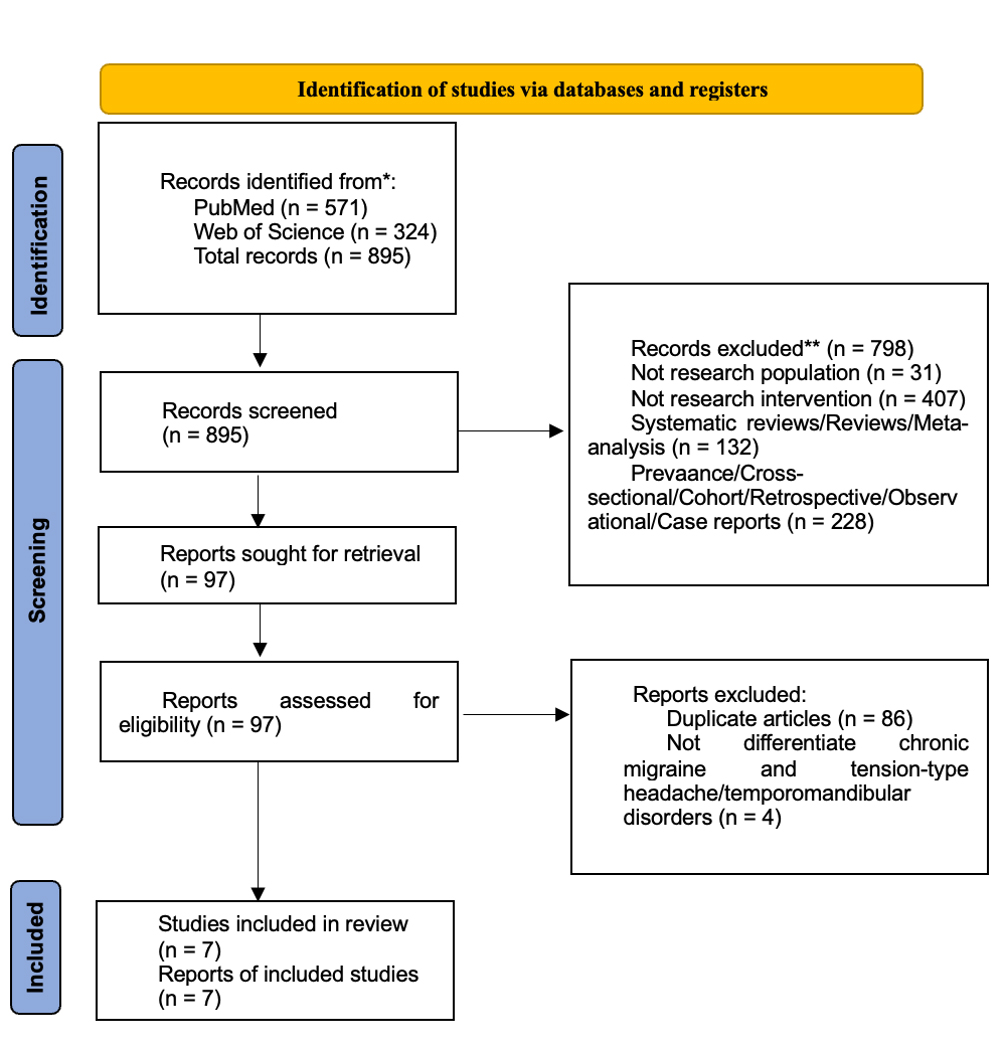 Fig. 1.
Fig. 1.PRISMA Flowchart Diagram of the Study. * Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). ** If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The included trials investigated various physical therapy and rehabilitation approaches for rehabilitation in chronic migraine patients. The specific interventions assessed in these studies were as follows: aerobic exercise [26], osteopathic manipulative treatment (OMT) [25], occipital transcutaneous electrical stimulation (OTES) [27], acupressure [23], hydrotherapy [21], instrument-assisted soft tissue mobilization (IASTM) [24], facial proprioceptive neuromuscular facilitation (FPNF), and connective tissue massage (CTM) [28]. The sample sizes in the different arms of the studies ranged from 15 to 49 patients, with a mean age ranging between 31 and 41.7 years. However, one study did not provide data on the age of the participants [21]. Most patients included in the studies were female, although two studies did not report data on the gender composition of their participants [21, 28]. A detailed summary of the study characteristics, including the interventions used, sample sizes, mean age, and sex distribution, can be seen in Table 1 (Ref. [21, 23, 24, 25, 26, 27, 28]).
| Study name | Country | Sample size, n | Age, mean |
%, Female | Intervention group | Control group | Tx period | Outcome measures |
| Cerritelli et al. 2015* [25] | Italy | I; 35 | I: 36.9 |
I: 77.1% | OMT and medical Tx | C: Medical Tx | 24 weeks | Quality of life (HIT-6) |
| C; 35 | C: 38.4 |
C: 57.1% | S: Sham and Medical Tx | Migraine days/month | ||||
| S; 35 | S: 40.7 |
S: 62.9% | Intensity of pain | |||||
| Functional disability (MIDAS) | ||||||||
| Santiago et al. 2014* [26] | Brazil | I; 24 | I: 31 |
I: 79% | Amitriptyline and aerobic exercise | Amitriptyline | 12 weeks | Headache frequency (days/month), Intensity of headache (1 (mild), 2 (moderate), and 3 (disabling)), Duration/day of headache (6 h, 12 h, 18 h, and 24 h) |
| C; 26 | C: 35 |
C: 88% | ||||||
| Sujan et al. 2016* [21] | India | I; 20 | N.A. | N.A. | Hydrotherapy and pharmacotherapy (NSAIDs: domperidone 10 mg, naproxen sodium 500 mg [NAXDOM]) (if needed) and prophylactic medication with flunarizine 10 mg daily | Pharmacotherapy (NSAIDs (domperidone 10 mg, naproxen sodium 500 mg [NAXDOM]) (if needed) and prophylactic medication with flunarizine 10 mg daily | 45 days | Quality of life (HIT-6) |
| C; 20 | Intensity of Headache (VAS) | |||||||
| Headache frequency (headache diary) | ||||||||
| Torlak et al. 2022* [24] | Turkey | I1; 15 | I1: 41.67 |
I1: 100% | I1: IASTM | No intervention | 5 weeks | Head and Neck Pain intensity: NPS |
| I2; 15 | I2: 37.2 |
I2: 100% | I2: OTES and Home exercise | And Home exercise | Quality of Life: HIT-6 and SF-36 | |||
| C; 15 | C: 39.87 |
C: 100% | ||||||
| Xu et al. 2017* [23] | China | I; 49 | I: 38.4 |
I: 71.4% | Acupressure and | Sodium valproate | 8 weeks | Intensity of pain (NRS) |
| C; 49 | C: 39.2 |
C: 77.5% | Sodium valproate | Migraine attacks (Frequency) | ||||
| Quality of Life (SF-36) | ||||||||
| Bono et al. 2015 |
Italy | I; 54 | I: 41 |
I: 88.9% | Real OTES | Sham OTES | 2 weeks | Intensity of pain (VAS) |
| C; 23 | C: 40 |
C: 69.6% | Disability (MIDAS) | |||||
| Kurt et al. 2022 [28] | Turkey | I; 20 | I: 35.15 |
N.A. | I: FPNF | C: CTM | 6 weeks | Intensity of pain (VAS) |
| C; 20 | C: 35 |
C, Control group; SD, Standard Deviation; TM, connective tissue massage; FPNF,
facial proprioceptive neuromuscular facilitation; HIT-6, Headache Impact Test-6;
I, Intervention group; I1, First intervention group; I2, Second intervention
group; IASTM, Instrument-assisted soft tissue mobilization; MIDAS, Migraine
Disability Assessment Test; N.A., not available; NPS, Neck Pain Scale (similar to
VAS); NSAIDs, nonsteroidal antiinflammatory drugs; OMT, osteopathic manipulative
treatment; OTES, occipital transcutaneous electrical stimulation; S, Sham group;
SF-36, Short Form 36; Tx, treatment; VAS, Visual Analog Scale; NAXDOM, naproxen
sodium; NRS, Numeric Rating Scale; CTM, connective tissue massage. *Trials included in the meta-analysis.
These studies assessed different outcomes and utilized various scales to evaluate the efficacy of physical therapy and rehabilitation approaches. The intensity of the headache was measured using different scales across the studies. One study used a rating scale with categories of “1-mild, 2-moderate, 3-disabling” [26], while others used the Visual Analog Scale (VAS) [21, 27, 28], Numeric Rating Scale (NRS) [23], and Neck Pain Scale (NPS), which is essentially a VAS evaluating both headache and neck pain [24]. The duration of headache was evaluated in only one study, where patients were asked to select among options of 6, 12, 18, or 24 hours of duration [26]. The frequency of headache was assessed in four studies, but the definition varied among the studies. This was measured as headache days per month in the studies by Santiago et al. [26] and Cerritelli et al. [25], migraine attacks in the study by Xu et al. [23], and through a daily headache diary in the study by Sujan et al. [21].
Disability related to headache was evaluated in two studies, both of which
utilized the Migraine Disability Assessment Scale (MIDAS) [25, 27]. QoL was
assessed in four studies, with two studies using the Short Form 36 (SF-36)
questionnaire [23, 24], and three studies employing the Headache Impact Test-6
(HIT-6) [21, 24, 25]. In the study by Santiago et al. [26], the efficacy
of amitriptyline alone was compared with the combination of amitriptyline and
aerobic exercise over a 12-week period. The findings showed significant
reductions in headache frequency (days per month) (p = 0.001), duration
of headache attacks (p = 0.017 for 6 hours, p = 0.001 for 12
hours, and p = 0.001 for 24 hours), and intensity of headache (p
= 0.048). These results support the benefit of adding aerobic exercise to
pharmacological therapy in the management of chronic migraine [26]. Cerritelli
et al. [25] examined the efficacy of OMT as a modality of physical
therapy in chronic migraine. The study aimed to evaluate the benefit of combining
OMT with medical therapy compared with medical therapy alone over a 24-week
period. The study design consisted of three treatment arms: OMT and medication
therapy, sham manipulative therapy and medication therapy, and medication therapy
alone. The results of the study indicated that the combination of OMT and
medication therapy had a positive impact on QoL. There was a statistically
significant decrease in HIT-6 scores (a measure of headache impact) in the OMT
and medication therapy arm compared with both the sham manipulative therapy and
medication therapy arm, as well as the medication therapy alone arm (p
In another study conducted by Sujan et al. [21], the effectiveness of
hydrotherapy combined with medical therapy was investigated in chronic migraine
patients over a period of 45 days. The results demonstrated significant decreases
in HIT-6 scores for frequency of headache and intensity of headache when compared
with medical therapy alone (p
In contrast, the study by Xu et al. [23] examined the impact of acupressure in addition to sodium valproate on chronic migraine. The treatment duration was 8 weeks, and the outcomes assessed included intensity of headache, frequency of migraine attacks, and QoL measured using SF-36. However, the results did not show a reduction in the intensity of headache, frequency of migraine attacks, or improvements in QoL compared with the use of sodium valproate alone. These findings suggest that acupressure as an adjunct to sodium valproate may not provide additional benefits in terms of intensity of headache reduction and overall QoL improvement [23].
In a recent study conducted by Torlak et al. [24], approaches involving IASTM and OTES were evaluated to test their effectiveness in chronic migraine patients. The treatment duration was 5 weeks. The results showed a significant decrease in the intensity of headache and neck pain in both the IASTM arm (p = 0.001, effect size = 0.78) and the OTES arm (p = 0.001, effect size = 0.82). Furthermore, the QoL was improved in both the IASTM arm (p = 0.01, effect size = 0.78) and the OTES arm (p = 0.01, effect size = 0.78) compared with the control arm, which did not receive any approach. However, there were no significant differences observed between the two interventions in terms of efficacy [24]. Bono et al. [27] also evaluated the effectiveness of OTES in improving chronic migraine and chronic tension-type headache. The intervention was administered for only 2 weeks and the study did not find statistically significant differences in disability scores and intensity of pain between real and sham stimulations [27].
Kurt et al. [28] evaluated the effectiveness of two interventions, FPNF and CTM, in patients with chronic migraine over a period of 6 weeks. Both interventions resulted in significant reductions in the intensity of headache (p = 0.001 for both), indicating their potential efficacy in managing chronic migraine. Importantly, no significant difference in effectiveness was observed between the FPNF and CTM interventions [28]. These findings suggest that both FPNF and CTM can be beneficial in reducing the intensity of headache in chronic migraine. Authors suggested that either intervention can be considered as a viable treatment option to manage chronic migraine [28].
Adverse events (AEs) associated with the physical therapy and rehabilitation approaches were reported in only one study [23]. Patients who underwent combined therapy with acupressure and sodium valproate experienced AEs such as nausea, diarrhea, hair loss, neck pain, flu-like syndrome, and pruritus. In contrast, patients who received only sodium valproate reported vomiting, worsening migraine, and back pain [23]. These findings highlight the importance of monitoring and managing potential AEs when implementing physical therapy and rehabilitation interventions in the management of chronic migraine. Healthcare providers should carefully evaluate the risks and benefits of such interventions and take appropriate measures to mitigate any potential side effects.
Data synthesis and analysis were performed on five out of the seven trials
included in the systematic review. A total of 183 patients from the studies
reporting changes in the intensity of headache [21, 23, 24] and 195 patients from
the studies reporting changes in headache days [21, 25, 26] were included in the
quantitative analysis. However, the data from the study that evaluated OTES [27]
were not included in the analysis, along with the data from the studies that
utilized manual physical therapies [21, 23, 24, 25]. Heterogeneity in terms of
intensity of headache and headache days per month was assessed using the I
Three trials provided data on the improvement of the intensity of headache, assessed using a VAS or NRS with scores ranging from 0 to 10. Among these RCTs, the methodological quality of the studies conducted by Xu et al. [23] and Torlak et al. [24] was graded as excellent with scores of 10 and 9, respectively (Table 2, Ref. [21, 23, 24, 25, 26, 27, 28]). The study by Sujan et al. [21] was deemed to have good methodological quality with a score of 6 (Table 2). All three studies included in the meta-analysis had good to excellent methodological quality.
| Author, year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
| Santiago et al., 2014 [26] | YES | YES | NO | NO | NO | NO | NO | YES | YES | YES | YES | 6 |
| Bono et al., 2015 [27] | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | 11 |
| Cerritelli et al., 2015 [25] | YES | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 9 |
| Sujan et al., 2016 [21] | YES | YES | NO | NO | NO | NO | NO | YES | YES | YES | YES | 6 |
| Xu et al., 2017 [23] | YES | YES | YES | YES | NO | YES | YES | YES | YES | YES | YES | 10 |
| Kurt et al., 2022 [28] | YES | YES | YES | YES | NO | NO | NO | YES | YES | YES | YES | 8 |
| Torlak et al., 2022 [24] | YES | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 9 |
Note that “YES” represents the presence of the item. “NO” represents the absence of the item.
1: Eligibility criteria were specified.
2: Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received).
3: Allocation was concealed.
4: The groups were similar at baseline regarding the most important prognostic indicators.
5: There was blinding of all subjects.
6: There was blinding of all therapists who administered the therapy.
7: There was blinding of all assessors who measured at least one key outcome.
8: Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups.
9: All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”.
10: The results of between-group statistical comparisons are reported for at least one key outcome.
11: The study provides both point measures and measures of variability for at least one key outcome.
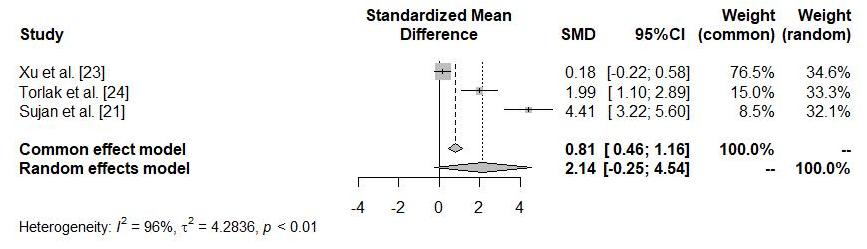
The random-effects model analysis showed that the standardized mean difference
(SMD) of the intensity of headache was higher in patients who received manual
physical therapy compared with those who did not receive it, although the
difference did not reach statistical significance (SMD: 2.14, 95% confidence
interval (CI): –0.25, 4.54; I
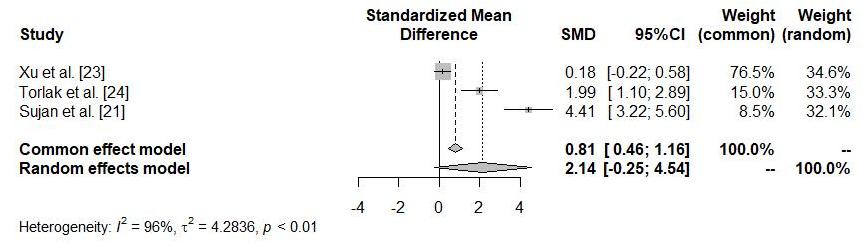 Fig. 2.
Fig. 2.Forest plot analysis of changes from baseline in the intensity of headache. SMD, standardized mean difference; CI, confidence interval.
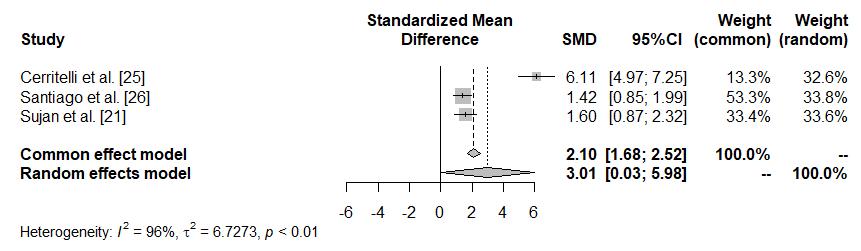
Three trials examined headache frequency as the number of headache days per
month. The study by Cerritelli et al. [25] was rated as excellent in
terms of methodological quality (score: 9), while the studies by Santiago
et al. [26] and Sujan et al. [21] were considered to have good
methodological quality (scores: 6 for both) (Table 2). All three studies included
in the meta-analysis of headache days had good to excellent methodological
quality. The random-effects model analysis revealed a significantly greater SMD
in patients who received manual physical therapy as an add-on to medical therapy,
compared with those who received medical therapy alone (SMD: 3.01, 95% CI: 0.03,
5.98; I
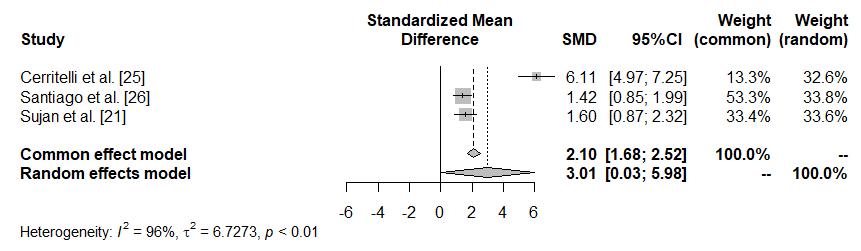 Fig. 3.
Fig. 3.Forest plot analysis of changes from baseline in headache days per month.
In the study by Santiago et al. [26], the methodological quality score was good (score: 6). However, this study was not included in the quantitative analysis because the outcome measure (intensity of headache) was evaluated using a different method compared with the studies included in the meta-quantitative analysis. The study conducted by Kurt et al. [28] also had a good methodological quality score (score: 8). This study was not included in the analysis because both groups in the study received active manual physical therapy approaches, and there was no control group. The study by Bono et al. [27] had an excellent methodological quality score (score: 11). However, data from the OTES were not included in the analysis of manual therapy data. Although these studies were not included in the quantitative analysis, their methodological quality was assessed, and the reasons for exclusion are provided. The results of the methodological quality assessments are shown in Table 2.
Our systematic review highlights the limited number of RCTs investigating the efficacy of physical therapy and rehabilitation approaches in chronic migraine. These trials employed various intervention arms, which included different modalities of physical therapy: aerobic exercise, OMT, OTES, acupressure, hydrotherapy, IASTM, FPNF, and CTM. Overall, the physical therapy and rehabilitation arms showed more favorable outcomes compared with the control or medical therapy alone arms. However, it is worth noting that the studies utilized different outcome measures, limiting the ability to directly compare the results. Our meta-analysis focused on changes in the intensity of headache and headache days, being the common outcome measures of some of these trials. The analysis revealed a significant improvement in the manual physical therapy add-on arm compared with the medical therapy alone arm for both intensity of headache and headache days per month.
Osteopathic manipulative treatment in conjunction with medication was shown to improve QoL and reduce disability, intensity of pain, and migraine days per month [25]. Similarly, FPNF and CTM [28] being other types of manual therapy approaches used in a recent trial, were effective to reduce the intensity of headache. Hydrotherapy combined with medication also resulted in improvements in intensity, frequency of headache, and overall QoL [21]. However, combination therapy with acupressure and sodium valproate did not improve the intensity and frequency of migraines, analgesic consumption, or QoL in comparison with the control group [23].
Occipital transcutaneous electrical stimulation is another physical therapy and rehabilitation approach used in migraine. The findings of a recent study suggest that both IASTM and OTES can effectively reduce the intensity of headache, alleviate neck pain, and improve the QoL in chronic migraine patients [24]. However, another study [27] could not show a similar effect, which may be attributed to the shorter intervention period of 2 weeks. Although studies on electrical stimulation specifically in the chronic migraine population are limited, previous research on head and neck pain has reported significant improvements in the intensity of pain when electrical stimulation was applied at intervals of 4–6 weeks [29, 30, 31]. These findings highlight the importance of the duration and frequency of OTES treatment in chronic migraine patients. Longer treatment periods and appropriate intervals between sessions seem to be necessary to achieve optimal therapeutic outcomes. Further research in the field is warranted to better understand the effectiveness of electrical stimulation in managing chronic migraine.
Aerobic exercise, combined with amitriptyline, was effective in reducing the intensity, frequency, and duration of headache, and improving psychological factors in patients with chronic migraine compared with amitriptyline alone [26]. Although physical activity can exacerbate headache during attacks [32], exercise has also been shown to increase well-being and reduce migraine symptoms [33]. However, the optimal aerobic exercise program for improving migraine related symptoms has not been clearly defined.
Exercise has been shown to increase beta-endorphin levels [34]. Beta-endorphin, known for its analgesic properties and thought to be released in response to stress, has been shown to be decreased in migraine patients compared with healthy individuals [35]. Moreover, patients with chronic migraine have even lower levels of beta-endorphin than those with episodic migraines [36]. Although studies specifically investigating beta-endorphin levels in chronic migraine patients and exercise are lacking, one study conducted an aerobic exercise program that involved exercising at 60% of the maximal heart rate, 3 days a week for 40 minutes a day, over a period of 6 weeks in migraineurs without aura. Following the exercise program, beta-endorphin levels nearly doubled and there were significant reductions in the intensity of headache, total duration per month, and number of attacks per month [37]. They reported also that migraineurs with low basal beta-endorphin levels experienced headaches with longer duration, suggesting that exercise may improve migraine symptoms in patients with low beta-endorphin levels [37]. From a vascular perspective, exercise is believed to have a prophylactic effect on migraine by reducing and regulating blood pressure [38]. Long-term, regular, and moderate aerobic exercise contributes to cardiovascular fitness and helps decrease the intensity, frequency, and duration of migraine attacks [39, 40]. Aerobic exercise increases cardiac output and promotes blood distribution to all body muscles. This increased mobility leads to elevated production of nitric oxide (NO) [39, 41]. In a study investigating the effects of aerobic exercise on NO levels in migraine patients without aura, the intervention group received submaximal aerobic exercise sessions 3 days a week for 60 minutes over an 8-week period, while the control group received drug treatment. The exercise group showed a significant increase in blood NO levels, a greater decrease in intensity of pain, and an increase in QoL in comparison with the control group. Consequently, aerobic exercise, through its effects on the circulatory system and relaxation of smooth muscles, can enhance well-being, alleviate problems such as intensity of pain, duration, and frequency, and improve symptoms in migraine patients [39]. Although there are several reports favoring aerobic exercise to reduce the intensity, duration, and frequency of attacks in migraine [42, 43], RCTs focusing on the optimal duration, frequency, and dosage of aerobic exercise are lacking [44].
Considering improvements in the intensity of headache and the number of headache days, manual therapy among other physical therapies and rehabilitation approaches stands out as a prominent approach due to its potential to modulate pain. During migraine attacks, neurogenic inflammation triggers the release of cytokines, which in turn stimulates the trigeminovascular system and activates neural pathways. These cytokines may contribute to central sensitization and the development of chronic pain by inducing neuroinflammation [45, 46, 47, 48]. Hypotheses regarding the effectiveness of manual therapy propose that it reduces the inflammatory response by acting on inflammatory cytokines, diminishes pain response by activating the parasympathetic system, and can lower pain perception [49] by targeting inhibitory systems at various levels in the spinal cord [50]. Manual therapy leads to vasodilation, increased blood flow, and muscle relaxation, thereby decreasing pain perception and promoting tissue relaxation. Consequently, manual therapy approaches exhibit a relaxing effect mediated by the parasympathetic system [50].
International guidelines on migraine prevention trials recommend specific outcome measures such as the change in migraine days, moderate/severe headache days, or the 50% responder rate for reducing migraine days [51]. However, in the studies included in this systematic review, only one study evaluated the number of migraine days per month [25], while another study assessed headache days per month [26]. It is important to note that Bono et al. [27] reported a 50% or more reduction in headache days per month, but their study group included both patients with chronic migraine and tension-type headache. Therefore, data regarding the 50% responder rate for reducing migraine days could not be obtained from these studies, and only the overall reductions in headache days per month and intensity of headache were evaluated. The quantitative analysis of the available data showed that manual therapy approaches or hydrotherapy combined with medication reduced the intensity of headache. Furthermore, manual therapy approaches, hydrotherapy, or aerobic exercise combined with medication significantly reduced the number of headache days per month. The duration of active treatment also varied across the included trials, ranging from 2 to 12 weeks. The results of the meta-analysis indicated that manual therapy approaches applied for 5–8 weeks, as well as pharmacological treatment combined with hydrotherapy, were associated with significant reductions in the intensity of headaches [21, 23, 24]. Similarly, manual therapy interventions applied for 6–24 weeks, along with amitriptyline treatment combined with aerobic exercise for 12 weeks, significantly reduced the number of headache days per month in chronic migraine patients [21, 25, 26]. All these findings suggest that physical therapy interventions, particularly manual therapy approaches, can be effective in alleviating symptoms and improving outcomes in chronic migraine. However, due to the heterogeneity in the interventions and outcome measures used across studies, caution should be exercised when interpreting the results.
The limited number of studies assessing the recommended outcome measures in accordance with the international guidelines highlights the need for future research to align with these recommendations. Consistency in outcome measures will enhance the comparability and generalizability of study results, allowing for more robust evidence synthesis and informed decision-making in clinical practice. Finally, while international guidelines recommend specific outcome measures for assessing migraine prevention trials, the studies included in this review deviated from these recommendations. Further research with standardized protocols and consistent outcome measures is needed to better understand the efficacy and optimal duration of physical therapy interventions for chronic migraine.
Physical therapy and rehabilitation approaches are generally safe interventions with few side effects when applied at the appropriate time, frequency, and dosage. In this review, only one study using acupressure and sodium valproate reported side effects [23] such as nausea, vomiting, diarrhea, neck-back pain, flu-like symptoms, or worsening migraine. Nonetheless, the overall safety profile of physical therapy and rehabilitation approaches in managing migraine appears to be favorable. However, it is crucial to consider the specific circumstances and individual characteristics of patients when implementing these interventions. Adherence to proper guidelines, professional supervision, and personalized treatment plans can further minimize the risk of adverse effects. It is important that healthcare providers closely monitor patients during treatment to ensure their well-being and promptly address any concerns or complications that may arise. Further research and evidence are also needed to comprehensively evaluate the safety and potential side effects of different physical therapy and rehabilitation approaches for migraine management.
Limited number of studies: The systematic review identified only seven RCTs that met the inclusion criteria, indicating a limited number of studies available on the topic. This could potentially limit the generalizability and robustness of the findings.
Heterogeneity among studies: The included studies varied in terms of study design, sample size, interventions, treatment duration, and outcome measures. This heterogeneity may introduce variability in the results and make it challenging to draw definitive conclusions.
Small sample sizes: Three out of seven trials randomized 20 or fewer patients in intervention arms. The largest sample included 54 patients in the intervention arm.
Lack of long-term follow-up: The duration of the interventions and follow-up periods in the included studies were relatively short, ranging from 2 weeks to 24 weeks. This short-term follow-up may not capture the long-term effectiveness and sustainability of physical therapy and rehabilitation approaches for chronic migraine.
Potential publication bias: The systematic review searched for studies in only two databases, which might have introduced publication bias. Relevant studies published in other languages or unpublished studies might have been missed, potentially leading to an incomplete representation of the evidence.
Methodological quality of included studies: The methodological quality of the included RCTs was assessed using the PEDro scale. While this scale is commonly used, it is important to note that it has some limitations and may not capture all aspects of study quality. Therefore, the overall quality of the included studies should be interpreted with caution.
Multidisciplinary approach: Our review highlights the need for a multidisciplinary approach in the management of chronic migraine, and indicates that healthcare professionals from different disciplines, such as neurology, physical therapy, and rehabilitation, should collaborate to provide comprehensive care for individuals with chronic migraine.
Non-drug interventions as adjunct treatments: Our findings emphasize the potential benefits of non-drug interventions, such as physical therapy and rehabilitation approaches, as adjunct treatments for chronic migraine when drug therapy is insufficient or associated with intolerable side effects. A combination of pharmacological and non-pharmacological interventions may offer a more comprehensive approach to managing chronic migraine.
Individualized treatment plans: Our study highlights the importance of tailoring treatment plans to individual patients, considering factors such as intensity, frequency, duration of headache, disability, and QoL. Healthcare providers should assess and consider the specific needs and characteristics of each patient when determining the most appropriate physical therapy and rehabilitation interventions.
Adverse event monitoring: We have discussed AEs associated with the physical therapy and rehabilitation interventions, indicating the importance of monitoring, and managing potential side effects. Healthcare providers should closely monitor patients undergoing these interventions and take appropriate measures to minimize AEs.
Further research: The limitations identified in our systematic review highlight the need for further research in this field. Future studies should aim to address the identified limitations, including conducting larger and more rigorous RCTs with longer follow-up periods, considering diverse populations, and exploring the comparative effectiveness of different physical therapy and rehabilitation approaches for chronic migraine.
Furthermore, it is worth noting that the methodological quality of the studies included in the analysis was generally good to excellent. This indicates that the results concerning the intensity of headache and frequency of headache days were supported by articles of high methodological quality.
In conclusion, upon reviewing the literature, it is evident that while medical treatment is typically the primary approach for managing chronic migraine patients, physical therapy and rehabilitation interventions tailored to the individual’s preferences, administered over an extended period, have shown significant reductions in the intensity of headache and frequency of headache days. However, several factors such as the specific content, duration, frequency, dosage, and sample size of these interventions, as well as the inclusion of different types of headaches within the patient population, contribute to the heterogeneity observed among the studies. Consequently, clear protocols for applying physical therapy and rehabilitation approaches to alleviate migraine symptoms in chronic migraine patients are currently lacking.
To address this gap, future studies should focus on RCTs involving larger sample sizes and longer treatment durations within the chronic migraine patient population. By doing so, the findings in the literature can be more reliably interpreted and clinicians and researchers can develop holistic approaches, including appropriate medical and physical therapies, and rehabilitation tools for the management of migraine.
The data used in this article were obtained from the articles included in the meta-analysis.
DO, HA, EE, AÖ and PM designed the researched study. DO, HA, and EE performed the research. BT analyzed the data. DO, HA, BT, EE, AÖ, and PM contributed to the writing of the article. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
The authors thank the Global Migraine Pain Society for the meta-analysis training support.
This research received no external funding.
Dilara Onan, Halime Arikan, Bahar Tasdelen and Paolo Martelletti declare no conflict of interest. Esme Ekizoglu received honoraria from Allergan-Abbvie. Esme Ekizoglu is associate editor for Archives of Neuropsychiatry. Aynur Ozge has Society Leadership/Board position as President–Global Migraine and Pain Society, Turkey; MENA Headache Group, Personal fees: Lecture honoraria–Novartis, Lilly, Abdi Ibrahim Ilac, Pfizer, Ilko Ilac, Ali Raif, Abbvie, Royalties/Licences: Springer book royalties. Relationship with scientific journals: Associate Editor–Frontiers in Neurology, Reviewer–Cephalalgia, Headache, Journal of Headache and Pain, Neurology, Neurological Sciences Neurophysiology.
The search strategy. PubMed: (chronic migraine) AND (exercise OR aerobic OR stabilization OR resistance OR strength OR endurance OR motor control OR range of motion OR isometric OR flexibility OR coordination OR balance OR yoga OR relaxation OR breathing OR taichi OR kiko) AND (pain intensity OR pain severity OR headache intensity OR headache severity OR disability OR quality of life) (chronic migraine) AND (massage OR mobilization OR manipulation OR mulligan OR manual therapy OR chiropractic OR osteopathic) AND (pain intensity OR pain severity OR headache intensity OR headache severity OR disability OR quality of life) (chronic migraine) AND (ultrasound OR TENS OR taping or kinesiotaping) AND (pain intensity OR pain severity OR headache intensity OR headache severity OR disability OR quality of life). Web of Science: TS = ((chronic migraine) AND (exercise OR aerobic OR stabilization OR resistance OR strength OR endurance OR motor control OR range of motion OR isometric OR flexibility OR coordination OR balance OR yoga OR relaxation OR breathing OR taichi OR kiko OR massage OR mobilization OR manipulation OR mulligan OR manual therapy OR chiropractic OR osteopathic OR ultrasound OR TENS OR taping or kinesiotaping) AND (pain intensity OR pain severity OR headache intensity OR headache severity OR disability OR quality of life))
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.