


 , Selçuk ÖZTÜRK 1, Tolga MEMİOĞLU 2, Mehmet İNANIR 2
, Selçuk ÖZTÜRK 1, Tolga MEMİOĞLU 2, Mehmet İNANIR 21 Cardiology Department, Konya City Hospital, 42020 Konya, Türkiye
2 Department of Cardiology, Faculty of Medicine, Izzet Baysal Training and Research Hospital, Bolu Abant Izzet Baysal University, 14280 Bolu, Türkiye
§Current address: Department of Cardiology, Faculty of Medicine, Izzet Baysal Training and Research Hospital, Bolu Abant Izzet Baysal University, 14280 Bolu, Türkiye.
Abstract
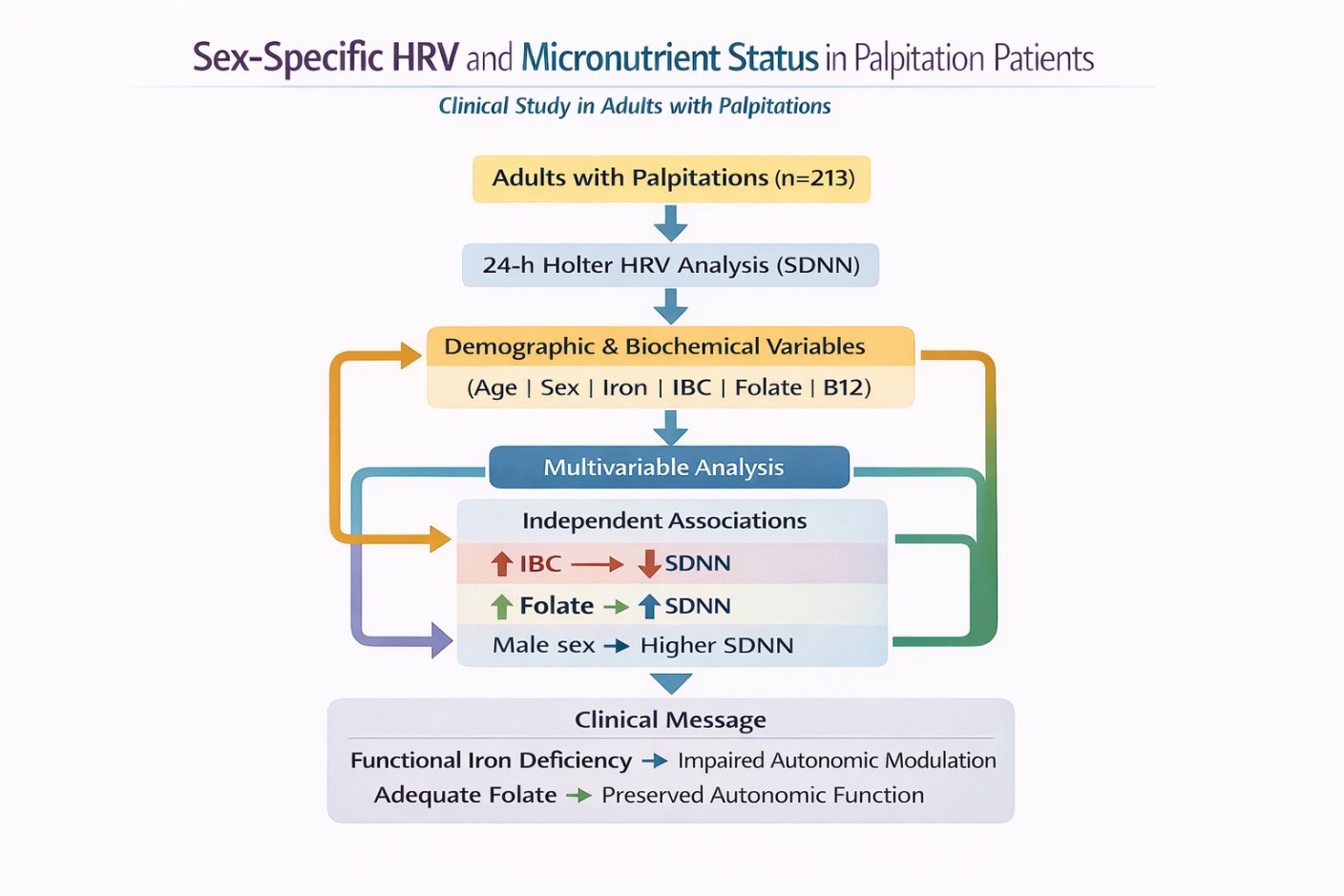
The sex-specific impact of micronutrient status on heart rate variability (HRV) in adults presenting with palpitations to cardiology outpatient clinics remains unclear. Thus, this study aimed to assess the demographic and biochemical determinants of HRV in a clinical cohort of patients presenting with complaints of palpitations.
This retrospective study included 213 adults aged 18–65 years who presented with palpitations and underwent 24-hour Holter monitoring at our institution between 2023 and 2024. Patients with cardiovascular disease, known arrhythmias, chronic inflammatory conditions, renal dysfunction, or use of medications that affected autonomic function were excluded from the study. Demographic variables, laboratory parameters, and HRV indices were statistically analyzed. The standard deviation of all normal-to-normal intervals (SDNN) was the primary HRV parameter used in both univariate and multivariate linear regression analyses.
The SDNN was significantly lower in women and older adults. In the univariate analyses, age (β = –0.203; p = 0.003), male sex (β = 0.529; p < 0.001), ferritin, serum iron, folate, and Vitamin B12 were all associated with the SDNN. However, in the multivariable model, only male sex (β = 0.467; p < 0.001), iron-binding capacity (IBC) (β = –0.377; p < 0.001), and folate (β = 0.117; p = 0.037) remained independent predictors. Elevated IBC, reflecting functional iron deficiency, was strongly associated with a reduced SDNN, whereas higher folate levels were associated with better autonomic modulation.
In patients presenting with palpitations, the SDNN is influenced by both demographic factors and biochemical markers of iron metabolism. Elevated IBC, reflecting alterations in iron metabolism and iron availability, was associated with impaired autonomic regulation, even in the absence of overt anemia. In contrast, adequate folate status appeared to support a more favorable autonomic function. These findings highlight the importance of integrating iron–vitamin assessment into the evaluation of autonomic function and underscore the need for prospective studies to determine whether correcting these abnormalities can improve HRV and clinical outcomes.
Graphical Abstract
Keywords
- autonomic nervous system
- ambulatory electrocardiography
- sex factors
- heart rate
- iron
- folic acid
- Vitamin B12
Palpitations, defined as abnormally rapid or irregular heartbeats, may present as skipped beats, fluttering, or a pounding sensation in the chest or neck. Although often benign, they can indicate life-threatening conditions. Palpitations can occur due to structural heart disease or systemic metabolic disorders; however, current knowledge regarding their effects on the autonomic nervous system is limited [1].
Heart rate variability (HRV) is a noninvasive marker of autonomic nervous system function. Reduced HRV is associated with adverse cardiovascular outcomes, including arrhythmias and increased mortality risk [2]. Sex differences in HRV exist, with women showing higher parasympathetic indices and men showing greater sympathetic modulation, indicating sex-specific autonomic regulation [3]. Recent studies have also highlighted autonomic dysfunction in outpatient populations with systemic or post-infectious conditions, emphasizing the clinical relevance of HRV assessment beyond overt cardiovascular disease [4]. Beyond autonomic tone, micronutrient status may also influence HRV. Vitamin B12 and folate are essential cofactors in one-carbon metabolism, and deficiencies can impair hematological and neurological function, potentially altering cardiac autonomic regulation [5]. In functional iron deficiency (FID), inflammation-induced hepcidin upregulation restricts iron availability for erythropoiesis despite adequate or increased iron stores. Unlike absolute iron deficiency, iron-binding capacity (IBC) does not exhibit a compensatory increase and should be interpreted in conjunction with other iron indices and the inflammatory milieu [6]. Combined deficiencies of Vitamin B12 and iron are frequently observed in clinical populations and are associated with distinct hematological and metabolic alterations that may have downstream effects on autonomic regulation [7]. Similarly, it has been shown that HRV is reduced in iron-deficient patients, and parasympathetic nervous system effects are impaired in iron-deficient individuals [8]. The common finding across these studies is that nutritional deficiencies adversely affect autonomic nervous system function and reduce HRV [9, 10, 11, 12]. Recent evidence highlights that sex-specific differences in vitamin metabolism and oxidative stress regulation may contribute to cardiometabolic health disparities, underscoring the importance of integrating nutritional biomarkers into cardiovascular risk assessment [13].
Despite these insights, few studies have simultaneously examined HRV in relation to sex differences and micronutrient status. Understanding these associations may provide novel perspectives on autonomic regulation and its interaction with nutritional deficiencies, particularly in patients with palpitations. Among HRV indices, standard deviation of all normal-to-normal intervals (SDNN) was selected as the primary outcome because it reflects overall autonomic modulation by integrating both sympathetic and parasympathetic influences and is widely accepted as a robust global measure of HRV in clinical and epidemiological studies. This study aimed to investigate sex-specific alterations in HRV and their associations with serum Vitamin B12, folate, and iron levels, thereby contributing to a more comprehensive understanding of cardiovascular risk stratification.
This retrospective observational study was conducted at Konya City Hospital, Türkiye, following approval by the Konya City Hospital Ethics Committee (Approval Date: 10.11.2025; Reference Number: 225/2025). Due to the retrospective design of the study, obtaining informed consent was not considered necessary. All procedures were performed in accordance with the ethical principles of the Declaration of Helsinki and its amendments. The funding bodies had no role in the study design, data collection, interpretation of the results, manuscript preparation, or statistical analyses.
A total of 580 adult patients who presented to the cardiology outpatient clinic with palpitations between 2023 and 2024 and underwent 24-hour rhythm Holter monitoring were screened. Patients were identified through the hospital electronic medical record system using the ICD-10 code R00.2 (palpitations). After applying the exclusion criteria, 213 patients aged 18–65 years were included in the final analysis.
To minimize confounding factors that could influence autonomic nervous system function, patients with the following characteristics were excluded:
● Age
● Known coronary artery disease, heart failure, prior revascularization, and/or coronary surgery.
● Acute coronary syndromes or documented arrhythmias.
● Known autonomic neuropathy.
● Use of any medications known to affect heart rate or autonomic function.
● Acute infectious or inflammatory conditions at the time of Holter monitoring.
● Moderate-to-severe renal impairment (creatinine
● Any chronic inflammatory disease or hematologic malignancy.
● Pregnancy.
After applying the exclusion criteria, 213 patients (113 women and 100 men) were included in the study cohort. Demographic characteristics, clinical variables, laboratory parameters, and 24-hour Holter-derived HRV indices were extracted from the hospital information system and recorded for statistical analysis.
Biochemical and laboratory data were obtained from the analysis of blood samples collected within the first 24 h of admission. Patients with missing hemogram and biochemistry data were excluded from the study.
All participants underwent 24-hour ambulatory electrocardiographic monitoring using the ‘Promedic digital ECG Holter system’. Continuous multichannel Electrocardiography (ECG) recordings were obtained during routine daily activities, and the participants were instructed to maintain their usual lifestyle throughout the monitoring period. Holter recordings were analyzed using manufacturer-provided software, which enabled the automated detection of R–R intervals and the calculation of HRV parameters. Automated beat classification was followed by a manual review to ensure the accurate identification of normal-to-normal (NN) intervals. Artifacts, ectopic beats, and noise were excluded from the analysis. Time-domain and frequency-domain HRV parameters were calculated from validated NN interval data in accordance with established international guidelines.
All statistical analyses were performed using the standard procedures for
observational cohort studies. Continuous variables are reported as mean
Correlations between HRV parameters and iron–vitamin biomarkers (ferritin, serum iron, IBC, folate, and Vitamin B12) were evaluated using Spearman’s rank correlation coefficients because of the non-normal distribution of HRV indices. Correlation analyses were performed for the entire cohort and separately for women and men.
A multivariable linear regression model was constructed to identify the
independent predictors of SDNN. Frequency-domain HRV parameters were analyzed in
their raw form as provided by the Holter analysis software, without logarithmic
transformation. Before multivariable linear regression, multicollinearity among
candidate variables was assessed using the variance inflation factor (VIF)
analysis, and no significant collinearity was detected. Variables were selected
for multivariable modeling based on clinical relevance and their observed
associations with SDNN in preliminary and univariate analyses (age, sex,
hemoglobin, CRP, ferritin, serum iron, IBC, Vitamin B12, and folate).
Standardized beta coefficients (
Statistical analyses were performed using IBM SPSS Statistics (version 27.0; IBM
Corp., Armonk, NY, USA) at a significance level of p
In total, 213 participants (n = 113, 53.1% women and n = 100, 46.9% men) were
included in the study. The distributions of the categorical demographic and
clinical variables are shown in Table 1. Smoking was significantly more common in
men than in women (15.5% vs. 6.6%, p
| All Cohort (n = 213) | Women (n = 113, 53.1%) | Men (n = 100, 46.9%) | p value | ||
| Smoking | 47 (22.1) | 14 (6.6) | 33 (15.5) | ||
| Hypertension | 18 (8.4) | 9 (4.2) | 9 (4.2) | 0.81 | |
| Diabetes | 9 (4.2) | 5 (2.3) | 4 (1.9) | ||
| Thyroid Dysfunction | 17 (8) | 11 (5.2) | 6 (2.8) | 0.46 | |
| Hypothyroid | 16 (7.5) | 10 (4.7) | 6 (2.8) | - | |
| Hyperthyroid | 1 (0.5) | 1 (0.5) | 0 (0) | - | |
| Iron Deficiency | 53 (24.9) | 49 (23) | 4 (1.9) | ||
| Vitamin B12 Deficiency | 22 (10.3) | 15 (7) | 7 (3.3) | 0.18 | |
| Folate Deficiency | 15 (7) | 12 (5.6) | 3 (1.4) | 0.034 | |
| Rhythm Holter Results | 213 (100) | 113 (53.1) | 100 (46.9) | 0.68 | |
| Sinus Tachycardia | 174 (81.7) | 94 (44.1) | 80 (37.6) | - | |
| Atrial or ventricular extrasystole | 29 (13.6) | 15 (7) | 14 (6.6) | - | |
| Paroxysmal atrial fibrillation | 10 (4.7) | 4 (1.9) | 6 (2.8) | - | |
Values are n (%). p values were calculated using Pearson’s chi-square test or Fisher’s exact test, as appropriate. Significant p values are shown in bold.
The continuous demographic, biochemical, and HRV parameters are summarized in
Table 2. Men had significantly higher levels of creatinine, AST, ALT, ferritin,
serum iron, and hemoglobin (all p
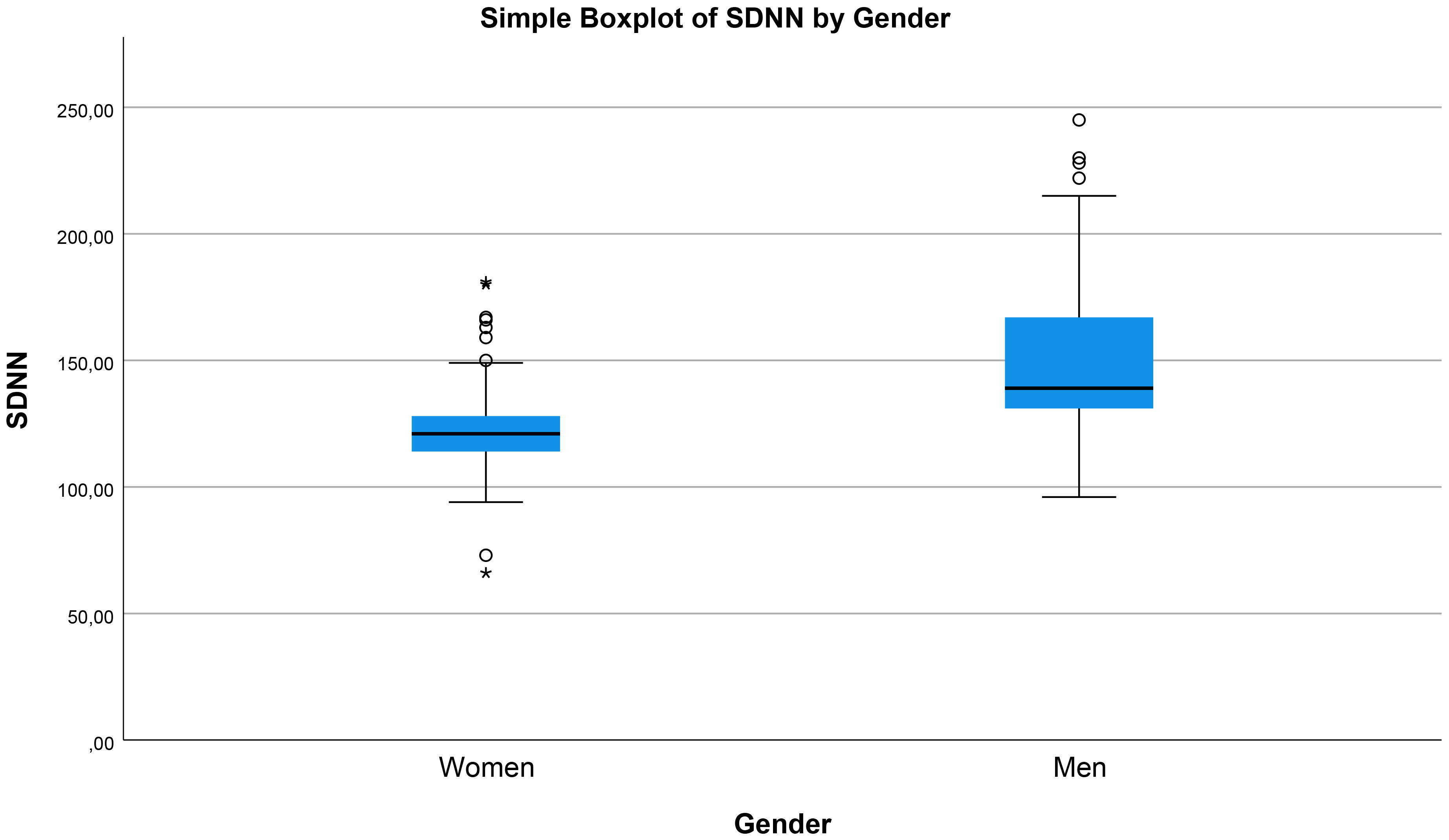 Fig. 1.
Fig. 1.
Box-and-whisker plot of 24-hour SDNN (ms) stratified by
sex, showing a higher median SDNN in men than in women. Outliers are displayed
as individual points; overall difference is significant (p
| All Cohort (n = 213) | Women (n = 113) | Men (n = 100) | p value | |
| Age, years | 34.46 |
34.14 |
34.84 |
0.68 |
| GLU, mg/dL | 94.63 |
93.69 |
95.7 |
0.55 |
| BUN, mg/dL | 11 (9–13) | 10 (9–12) | 12 (10–13) | |
| CRE, mg/dL | 0.71 (0.63–0.84) | 0.67 (0.61–0.75) | 0.79 (0.69–0.92) | |
| AST, U/L | 17 (15–20) | 16 (14–19) | 19 (15.25–22) | |
| ALT, U/L | 17 (12–22) | 14 (11–19) | 20 (15–29.75) | |
| TSH, mU/L | 2.06 |
2.21 |
1.88 |
0.16 |
| CRP, mg/L | 1.65 |
1.58 |
1.74 |
0.34 |
| Ferritin, ng/mL | 30 (15–66.5) | 20 (8–38.5) | 50.5 (29–81.75) | |
| Iron, µg/dL | 56 (38.5–91.5) | 44 (25.5–73) | 76.5 (52–101) | |
| IBC, µg/dL | 295 (249–367.5) | 331 (271–414) | 270.5 (235.5–309) | |
| Vitamin B12, pg/mL | 288 (244–375) | 299 (236.5–417.5) | 278 (247.5–345.75) | 0.151 |
| Folate, ng/mL | 6.69 |
6.63 |
6.74 |
0.78 |
| WBC, ×103/µL | 7.67 |
7.63 |
7.71 |
0.72 |
| HB, g/dL | 13.7 (12.65–15.3) | 12.8 (12–13.65) | 15.2 (13.9–16.4) | |
| Mean_HR, bpm | 79 (73–84) | 81 (77–85) | 77 (69–80.75) | |
| Lowest_HR, bpm | 50 (45–54) | 52 (48–56) | 46 (43–51) | |
| Highest_HR, bpm | 142.5 |
145.9 |
138.67 |
0.001** |
| SDNN (24 h), ms | 129 (119–144) | 121 (114–128) | 139 (131–167) | |
| SDNN-INDEX (24 h), ms | 50 (41–62) | 44 (37–49) | 59 (51.25–75) | |
| rMSSD, ms | 31 (26–36) | 29 (25–34) | 32 (26.25–44) | |
| pNN50, (%) | 14 (11–18) | 14 (9–16.5) | 15 (12–21) | |
| TRIANGULAR INDEX (24 h) | 22 (17.5–28) | 18 (16–23) | 26 (22–32.75) | |
| HF, ms2 | 486.9 (419.25–650.25) | 573.4 (394.65–650.25) | 467.45 (42.66–648.35) | 0.762 |
| LF, ms2 | 632.1 (496.45–716.8) | 541.9 (463.6–646.8) | 686.45 (628.65–906.93) | |
| VLF, ms2 | 1166.9 (773.05–1534.55) | 871.2 (673.65–1082.8) | 1532.7 (1426.1–1609.58) | |
| LF/HF | 1.21 (0.98–1.52) | 1.04 (0.94–1.19) | 1.46 (1.25–1.64) |
Continuous variables are reported as mean
*Significant at p
**Significant at p
GLU, Glucose; BUN, Blood Urea Nitrogen; CRE, Creatinine; AST, Aspartate aminotransferase; ALT, Alanine aminotransferase; TSH, Thyroid-Stimulating Hormone; CRP, C-Reactive Protein; IBC, Iron-Binding Capacity; WBC, White Blood Cell Count; HB, Hemoglobin; Mean_HR, Mean Heart Rate; SDNN, Standard Deviation of all normal-to-normal Intervals; SDNN-INDEX, Mean of the Standard Deviations of NN intervals for all 5-minute segments; rMSSD, root Mean Square of Successive Differences; pNN50, Percentage of successive NN Intervals differing by more than 50 ms; HF, High-Frequency; LF, Low-Frequency; VLF, Very-Low-Frequency; LF/HF, Low-to-High Frequency.
The Spearman correlation coefficients for the entire cohort are presented in
Table 3. All major time-domain HRV parameters (SDNN, SDNN-INDEX, rMSSD, pNN50,
TRIANGULAR INDEX) showed significant correlations with ferritin, serum iron, IBC,
folate, and Vitamin B12 (p
| HRV Parameters | Ferritin (ρ) | Iron (ρ) | IBC (ρ) | Folate (ρ) | Vit. B12 (ρ) |
| SDNN (24 h), ms | 0.314** | 0.272** | 0.210** | 0.162* | 0.148* |
| SDNN-INDEX (24 h), ms | 0.291** | 0.249** | 0.192** | 0.158* | 0.139* |
| rMSSD, ms | 0.278** | 0.244** | 0.189** | 0.151* | 0.132* |
| pNN50, (%) | 0.265** | 0.238** | 0.183** | 0.146* | 0.128* |
| TRIANGULAR INDEX (24 h) | 0.301** | 0.263** | 0.203** | 0.161* | 0.142* |
| LF/HF | 0.198** | 0.174* | 0.142* | 0.119 | 0.103 |
Positive correlation coefficients indicate higher HRV values with higher
micronutrient levels. Spearman’s rank correlation coefficient (
Sex-stratified-analyses revealed distinct patterns. Notably, correlation
coefficients between HRV parameters and iron–vitamin biomarkers were
approximately two-fold higher in women than in men, indicating a stronger
association between micronutrient status and autonomic modulation in female
participants (Tables 4,5). In men, the correlations between HRV indices and
iron–vitamin biomarkers were modest, reaching significance mainly for ferritin
and serum iron. In contrast, women exhibited consistently stronger correlations
across all HRV parameters, particularly with ferritin, iron, IBC, folate, and
Vitamin B12 levels (all p
| HRV Parameters | Ferritin (ρ) | Iron (ρ) | IBC (ρ) | Folate (ρ) | Vit. B12 (ρ) |
| SDNN (24 h), ms | 0.228* | 0.204* | 0.171 | 0.148 | 0.132 |
| SDNN-INDEX (24 h), ms | 0.213* | 0.192 | 0.163 | 0.139 | 0.127 |
| rMSSD, ms | 0.205* | 0.187 | 0.158 | 0.135 | 0.121 |
| pNN50, (%) | 0.198* | 0.179 | 0.152 | 0.129 | 0.116 |
| TRIANGULAR INDEX (24 h) | 0.219* | 0.196 | 0.167 | 0.142 | 0.129 |
| LF/HF | 0.162 | 0.148 | 0.131 | 0.118 | 0.104 |
Positive correlation coefficients indicate higher HRV values with higher
micronutrient levels. Spearman’s rank correlation coefficient (
| HRV Parameters | Ferritin (ρ) | Iron (ρ) | IBC (ρ) | Folate (ρ) | Vit. B12 (ρ) |
| SDNN (24 h), ms | 0.412** | 0.379** | 0.296** | 0.241* | 0.218* |
| SDNN-INDEX (24 h), ms | 0.398** | 0.361** | 0.284** | 0.229* | 0.204* |
| rMSSD, ms | 0.385** | 0.347** | 0.271** | 0.218* | 0.196* |
| pNN50, (%) | 0.371** | 0.336** | 0.263** | 0.211* | 0.189* |
| TRIANGULAR INDEX (24 h) | 0.403** | 0.368** | 0.287** | 0.236* | 0.213* |
| LF/HF | 0.241* | 0.218* | 0.179 | 0.152 | 0.138 |
Positive correlation coefficients indicate higher HRV values with higher
micronutrient levels. Spearman’s rank correlation coefficient (
Univariate regression analyses demonstrated that age was negatively associated
with SDNN (
| Univariate Analysis | Multivariate Analysis | Interpretation | ||||
| Standardized Coefficients | p-value | Standardized Coefficients | 95.0% Confidence Interval for B | p-value | ||
| Beta (ß) | Beta (ß) | [95% CI] | ||||
| Age | –0.203 | 0.003* | −0.269 | −0.88 to −0.34 | SDNN decreases with age | |
| Gender | 0.529 | 0.467 | 18.5 to 33.5 | SDNN is higher in men | ||
| HB, g/dL | 0.40 | −0.052 | −3.11 to 1.55 | 0.51 | Not significant | |
| CRP, mg/L | –0.088 | 0.202 | −0.035 | −3.39 to 1.77 | 0.53 | Not significant |
| Ferritin, ng/mL | 0.313 | −0.048 | −0.12 to 0.06 | 0.50 | Not significant | |
| Iron, µg/dL | 0.345 | −0.074 | −0.15 to 0.05 | 0.34 | Not significant | |
| IBC, µg/dL | –0.448 | −0.377 | −0.18 to −0.06 | Higher IBC → lower SDNN | ||
| Vitamin B12, pg/mL | 0.052 | 0.448 | 0.056 | −0.01 to 0.02 | 0.30 | Not significant |
| Folate, ng/mL | 0.097 | 0.159 | 0.117 | 0.06 to 2.11 | 0.037* | Higher folate → higher SDNN |
*Significant at p
In the present study, we observed marked sex-specific differences in HRV
parameters, with women demonstrating significantly lower time- and
frequency-domain indices (SDNN, rMSSD, pNN50, Low-Frequency (LF) Power, and
Very-Low-Frequency (VLF) Power) than men. This is consistent with prior
observations of sex differences in autonomic cardiac regulation, in which men
typically exhibit higher overall HRV, reflecting greater autonomic flexibility
[3, 14]. Multivariable regression analysis further confirmed that male sex was
independently associated with higher SDNN (
Iron deficiency was significantly more prevalent in women (23% vs. 1.9%,
p
Likewise, folate deficiency was more common in women (5.6% vs. 1.4%,
p = 0.034), with positive correlations between HRV indices and folate
levels, which were stronger in females than in males. Folate independently
predicted higher SDNN in the regression analysis (
Mechanistically, these micronutrients contribute to erythropoiesis, redox balance, and neurotransmitter synthesis, and deficiencies may promote sympathetic dominance, as evidenced by higher LF/HF ratios in deficient states. Sex disparities likely stem from reproductive factors that increase the deficiency risk in women, amplifying the autonomic effects [19]. Despite the non-significant association with CRP, subclinical inflammation cannot be fully excluded.
This study has several limitations related to its design, patient population, and single-center nature.
● Its retrospective design precludes causal inference, and unmeasured confounders may still be present despite the strict exclusion criteria.
● Although ferritin, iron, and inflammatory markers were evaluated, ferritin can be influenced by subclinical inflammation, and more sensitive inflammatory biomarkers (e.g., IL-6 and hepcidin) were not available in the dataset used.
● In addition, detailed information on dietary intake and micronutrient supplementation was not available, which may have influenced circulating iron, folate, and Vitamin B12 levels.
● HRV parameters were derived from 24-hour Holter recordings, which provide a robust assessment of autonomic function but may still be influenced by daily activity patterns, sleep quality, and psychological stress, factors that cannot be fully standardized or quantified retrospectively.
● The study population consisted of individuals presenting with palpitations, which may limit the generalizability of the results to asymptomatic or community-based populations. The study population may not be representative of the general population, limiting the generalizability of the findings.
● Finally, although the sample size was adequate for multivariable modeling, the inclusion of additional biochemical markers or longitudinal follow-up could further strengthen the mechanistic interpretation of the findings.
In this cohort of adults presenting with palpitations, SDNN, a key marker of global autonomic modulation, was strongly influenced by age, sex, and biochemical indices of iron metabolism. Male sex and younger age were associated with higher SDNN values, underscoring the importance of demographic stratification when interpreting HRV metrics in clinical settings. Although ferritin, serum iron, folate, and Vitamin B12 showed significant correlations with HRV parameters, only IBC and folate remained independent predictors in the multivariate analysis. These findings suggest that alterations in iron metabolism, reflected by elevated IBC, may impair autonomic regulation even in the absence of overt anemia, whereas adequate folate status may support healthier autonomic function.
Overall, our results highlight the need to consider demographic, biochemical, and nutritional factors when evaluating HRV in patients with palpitations. Identifying modifiable biochemical factors that influence HRV may offer opportunities for early intervention in patients with palpitations. Moreover, the strong effects of age and sex emphasize the need for demographic adjustments when interpreting HRV metrics in clinical settings. Given the retrospective observational design, the associations observed in this study do not imply causality. Therefore, no conclusions can be drawn regarding the potential benefits of iron or folate supplementation, which should be evaluated in future prospective and interventional studies. Future prospective studies are warranted to clarify the mechanistic pathways linking iron homeostasis and autonomic balance and to determine whether correcting iron handling-abnormalities or folate deficiency can improve HRV and clinical outcomes.
ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; BUN, Blood Urea Nitrogen; CRE, Creatinine; CRP, C-Reactive Protein; ECG, Electrocardiography; GLU, Glucose; HB, Hemoglobin; HF, High-Frequency; HR, Heart Rate; HRV, Heart Rate Variability; IBC, Iron-Binding Capacity; LF, Low-Frequency; LF/HF, Low-to-High Frequency; NN, Normal-to-Normal Intervals; Mean_HR, Mean Heart Rate; pNN50, Percentage of successive NN Intervals differing by more than 50 ms; rMSSD, root Mean Square of Successive Differences; SDNN, Standard Deviation of all NN Intervals; SDNN-index, Mean of the Standard Deviations of NN intervals for all 5-minute segments; TSH, Thyroid-Stimulating Hormone; VLF, Very-Low-Frequency; WBC, White Blood Cell Count.
The data used in this study are available upon reasonable requests.
The manuscript was conceived by MÖ, SÖ. The data were collected and the images and tables were prepared by MÖ and SÖ. MÖ, SÖ, TM, and Mİ were responsible for data analysis, statistical analysis, and interpretation of the results. The manuscript was written by MÖ, SÖ, TM, and Mİ. TM and Mİ critically revised the manuscript for important intellectual content. The entire process was supervised by MÖ and SÖ. The final version of the manuscript was carefully reviewed and approved by all authors, and all authors agree to be accountable for all aspects of the work.
The study was conducted in accordance with the principles of the Helsinki Declaration and approved by the Konya City Hospital Ethics Committee (decision number 225/2025, dated November 10, 2025, meeting number 2025/11). Due to the retrospective design of the study, obtaining informed consent was not deemed necessary.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
The graphical abstract was prepared using GPT-5.2 and OpenAI. The authors performed the study design, data analysis, and interpretation of results.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.