- Academic Editor
-
-
-
†These authors contributed equally.
Background: Exercise capacity reflects the cardiovascular risk after
myocardial infarction (MI). The study aims to evaluate the impact of
sleep-disordered breathing (SDB) on exercise capacity after MI. Methods:
Consecutive patients referring to outpatient cardiac rehabilitation up to 28 days
after MI and participating in the Polish Managed Care after Acute Myocardial
Infarction (MC-AMI) program were included. On admission, we assessed the presence
and the severity of SDB using the home sleep apnea test (HSAT), patients’ maximum
exercise capacity on a treadmill exercise stress test (EST), and a 6-minute walk
test (6MWT), as well as the effect of SDB on the results obtained. In the
multivariate analysis, we verified the strength of the observed associations
concerning age, anthropometric parameters, and left ventricular ejection fraction
(LVEF). Results: A total of 254 patients aged 60.00 (interquartile range
51.00–67.00), including 39 (15.4%) women, with technically adequate HSAT,
constituted the study group. Mild SDB was found in 82 (32.3%), moderate in 54
(21.3%), and severe in 51 (20.1%) patients. Among those diagnosed with SDB,
obstructive sleep apnea (OSA) was dominant in 167 (89.8%). With the worsening of
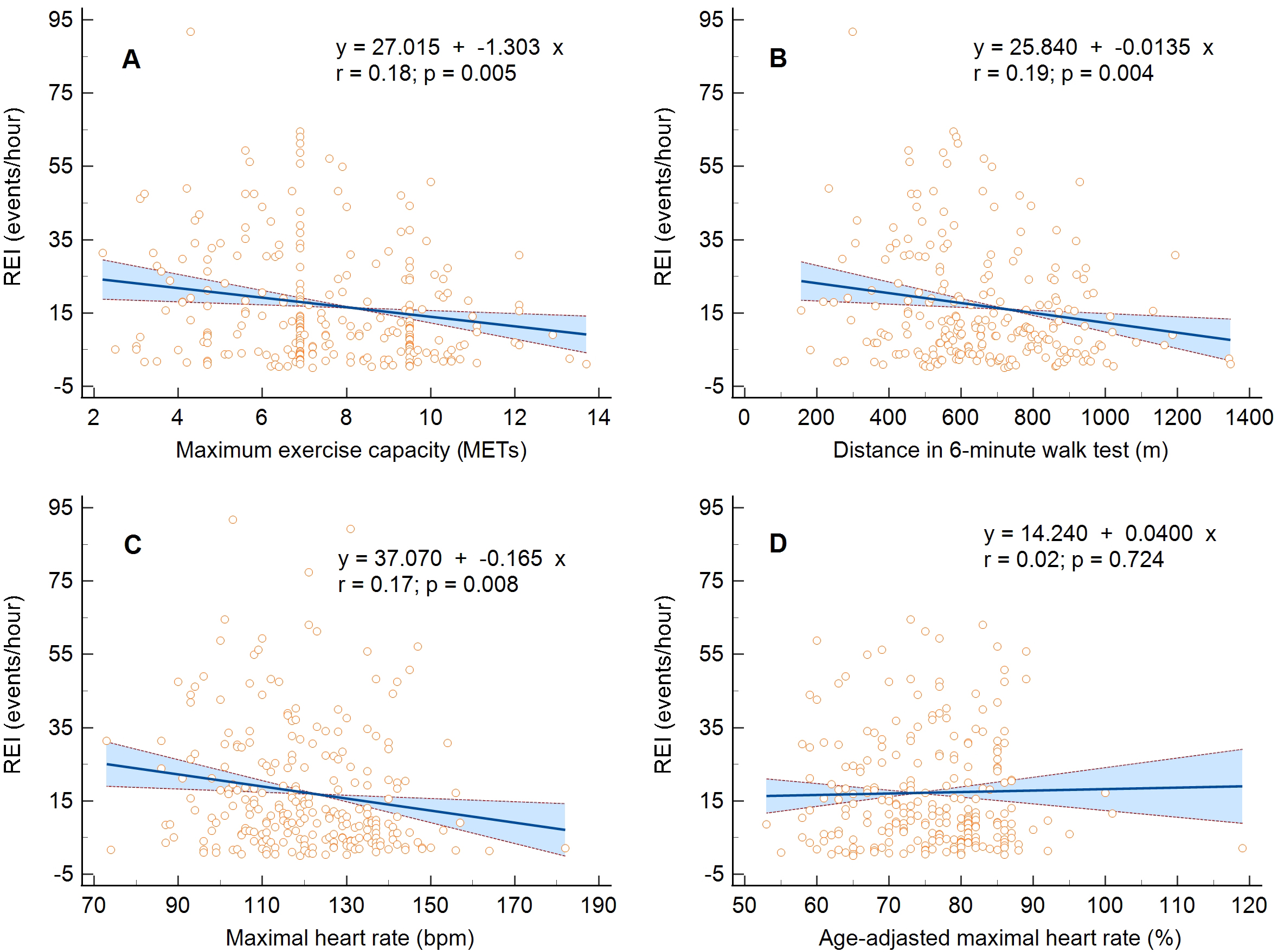
SDB, the distance in 6MWT and the maximum physical exertion achieved in EST,
expressed in metabolic equivalents (METs) and maximal heart rate (MHR),
decreased. The linear regression analysis confirmed the following: (1) inversely
proportional relationship between the respiratory event index and METs, MHR, and
6MWT distance (p = 0.005, p = 0.008, and p = 0.004),
and the maximum apnea duration and MET and 6MWT distance (p = 0.042 and
p = 0.002); and (2) directly proportional relationship between mean
arterial oxygen saturation (SpO