Background: Mitral regurgitation (MR) has a high prevalence and
aggravates hypoperfusion and hypoxia in heart failure (HF). Renal tubular
epithelial cells are sensitive to hypoxia, and therefore tubulointerstitial
damage is quite common in HF. However, the correlation between tubular
dysfunction and MR has not been studied. The aim of this work was to evaluate the
prognostic significance of urinary N-acetyl--d-glucosaminidase (uNAG), a
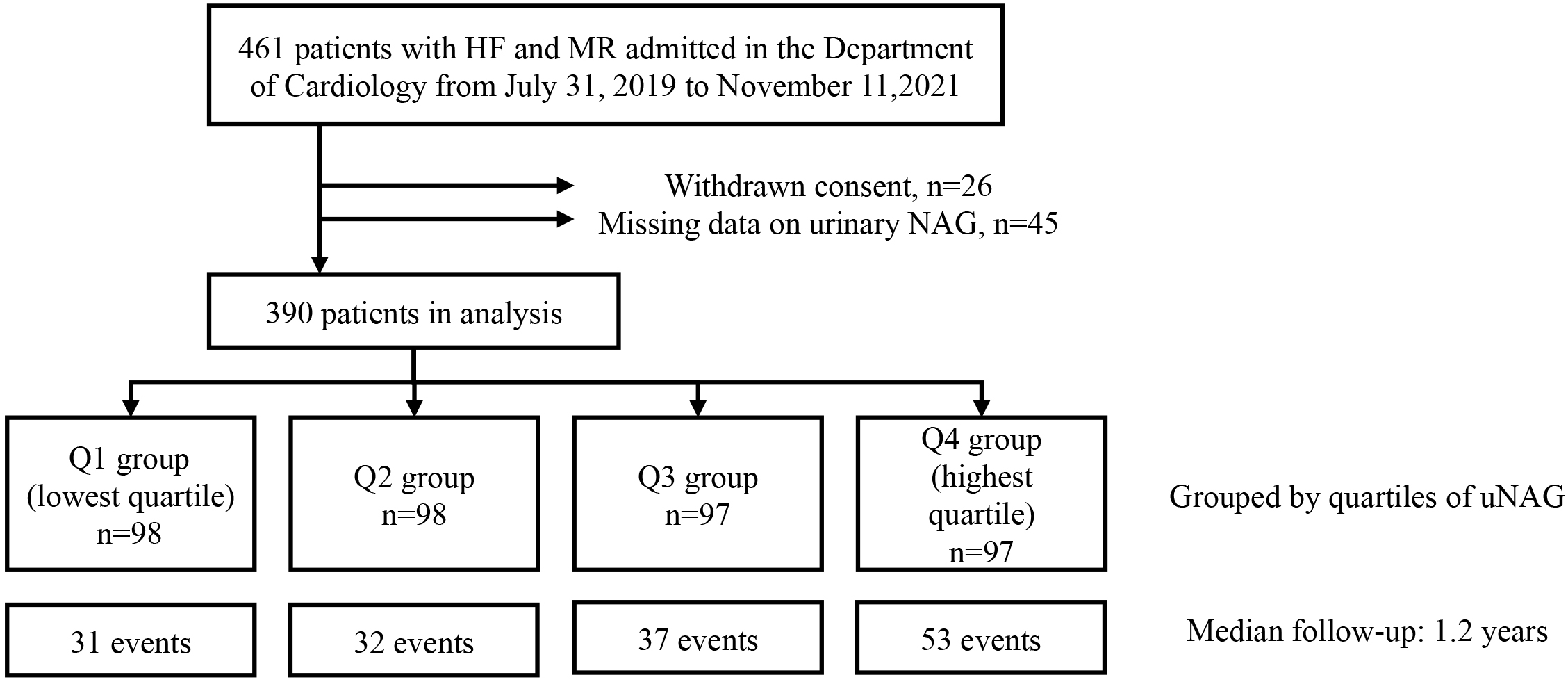
biomarker of renal tubular damage, in patients with HF and MR. Methods:
This was a prospective cohort study of 390 patients (mean age 64 years; 65.6%
male) with uNAG measurement on admission (expressed as urinary NAG/urinary
creatinine) and at least 1 year of follow-up data. The pre-defined primary
endpoint was the composite of all-cause mortality or rehospitalization for HF
after discharge. Cox regression analysis, restricted cubic splines, and subgroup
analysis were used to investigate the prognostic value of uNAG modeled as a
categorical (quartiles) or continuous (per SD increase) variable.
Results: A total of 153 (39.23%) patients reached the composite
endpoint over a median follow-up time of 1.2 years. The uNAG level correlated
with the severity of HF and with the incidence of adverse events. In a
multivariable Cox regression model, each SD (13.80 U/gCr) of increased
uNAG was associated with a 17% higher risk of death or HF rehospitalization
(95% confidence interval, 2–33%, p = 0.022), and a 19% higher risk
of HF rehospitalization (p = 0.027). Subgroup analysis revealed the
associations between uNAG and poor prognosis were only significant in younger
patients (65 years) and in patients without obvious cardiovascular
comorbidities. Conclusions: uNAG levels at admission were associated
with the risk of adverse outcomes in patients with HF and MR. Additional studies
are needed to further investigate the heart-kidney interaction.